Accurate Indicators of the Need to Go for Hepatitis B Treatment

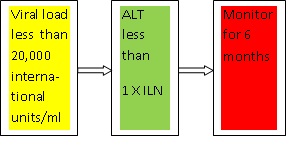
Accurate indicators, viral load and ALT, at their threshold levels. Below threshold, just monitor; above threshold, give treatment
DNA infectious particles are well protected by core protein and capsid that is why the risk of relapse in chronic hepatitis B carriers

Viral load and alanine amino transferase show more accurately that treatment for hepatitis B is needed
Common sense
Common senses says that when you had just been infected with hepatitis B virus you have acute hepatitis B. That is in about 3 to 4 months. Sometimes you feel the symptoms like flu-like, fatigue, jaundice and nausea. Other times you don’t feel any symptoms at all, that is called asymptomatic. So you do not know whether you have hepatitis B or not.
During acute hepatitis B your immune system fights back and it may succeed in bringing down the population of hepatitis B virus. However, the virus is not altogether defeated and you may go into what is called a window period. Here, blood test will not show positive for hepatitis B. However, blood test will show antibodies against the hepatitis early protein (HBeAg) and antibodies against the hepatitis core protein (HBcAg).
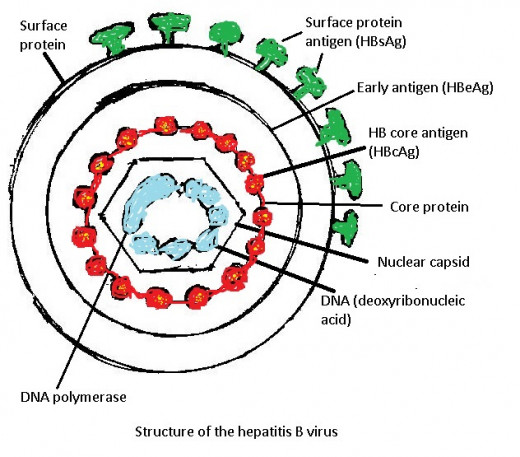
(You can review the structure of hepatitis B in my Hub “How to Treat a Person Who Had Acute Hepatitis B, Window Period, then Chronic Hepatitis B”).
Here’s the catch. A person infected by hepatitis B and gets well does not get rid of the virus. Even when he is vaccinated. Chronic hepatitis B comes in six months if the patient is not treated. That is why Offit and co-author in their book “Vaccines: What Every Parent Should Know” advise that blood test should be done after six months after treatment. In this period blood test will catch antigens for the surface protein (HBsAg), antibodies against the surface protein (IgG anti HBs) and antibodies against the core protein (IgG anti-HBc).
Let us recall that acute hepatitis B or chronic hepatitis B are not measures of the population of hepatitis B virus. They only show the length of time one had been infected with the virus. Acute means short time after infection; chronic means long time after infection.
In some countries or states, vaccination for hepatitis B is mandated. A baby born to a mother with hepatitis B should be vaccinated. The reason is that the virus in the mother’s blood infect the baby during delivery.
Common sense says that a baby by a mother with hepatitis B should be vaccinated. A person who had just been infected, within 70 hours, should be vaccinated. A person with chronic hepatitis B should be vaccinated or given a shot of immunoglobulin. However, bear in mind that hepatitis B cannot be eliminated altogether. We will get back to this topic later.
Accurate indicators
Besides common sense, you want accurate indicators when to get treated against hepatitis B. These indicators are: viral load and ALT (alanine amino transferase).
Viral load is counted as copies of virus per milliliter of blood. For example, 8 million copies per ml of blood.
ALT is an enzyme that is released by a cell killed during the battle by a component of the immune system, like T-Killer cell, and the virus. At this time, acute hepatitis B, inflammation occurs. This enzyme is detected by blood test. A gadget employing DNA PCR (deoxyribonucleic acid polymerase chain reaction) counts the virus contained in the blood.
[I am using ordinary language in describing this gadget. Suffice it to say that we now have this modern gadget that can give results in 4 to 5 days. ]
ALT is like the enzyme used to detect heart attack: MB fraction creatine kinase (CK-MB). The "heart muscle is the only tissue in the body containing more than 5 percent of CK-MB" (Clayman, C., MD. editor. Your Heart. 1989:62). Heart muscles that die owing to heart attack release CK-MB. Sometimes a heart attack does not immobilize or paralyze the victim but the presence of high amount of CK-MB in his blood indicates that he had a heart attack. High amount of CK-MB persists even a week after the attack.
In early 2000s, Taiwan made a study of reliable indicators of hepatitis B as bases for treatment. This study lasted for 15 years (Steven-Huv Han. Hepatitis B- Treatment and Consequences. Youtube. April 19,2014). Thus, viral load and ALT have been identified as indicators. After their identification several drugs for hepatitis B have been formulated.
Sequence of indicators
Viral load is less than 20,000 international unit/milliliter of blood, and alanine amino transferase is less than 1 X ILN, then monitor for six months. (See diagram above).
This sequence is adopted from Dr. Steven-Huv Han. It shows that when the viral load is less than 20,000 international unit per milliliter of blood, and the amount of alanine amino transferase is less than 1 x ILN, just monitor hepatitis B in six months. That is, no treatment is given.
However, when the viral load increases beyond 20,000 IU/ml and ALT also increases, treatment must be given.
It goes without saying that if the viral load is about 10,000 IU/ml treatment is no longer needed.
Consumer wants zero viral load
A consumer likes that his/her viral load is zero after treatment. However, that is impracticable and unnecessary. Why?
Hepatitis B consists of surface protein and DNA infectious particles contained in the capsid. The surface protein is not infectious and can be separated from the DNA infectious particle. There are more surface proteins (50 trillion per teaspoon of blood) than there are DNA infectious particles (500 million per teaspoon of blood), according to Offit and co-author (Offit, P., MD and L. Bell, MD. Vaccines: What Every Parent Should Know. 1996: 77-79).
If you extrapolate this ratio (100,000 surface protein is to one DNA infectious particle), a count of 10,000 IU/ml is a count for surface proteins. Not of DNA infectious particles. However, blood test detects both surface protein and DNA infectious particle.
Zero count by blood test is impracticable because this test will always catch a surface protein. To recall, surface protein is not infectious and does not replicate. Zero count is unnecessary because, at below 20,000 IU/ml or 10,000 IU/ml DNA infectious particles no longer exist.
Dr. Arturo V. Estuita, MD, a Filipino internist and chelationist, treats hepatitis B with chelation therapy. He reduces the viral load to 10,000 IU/ml then stops treatment. The reason is that the viral load is already stable, that is, the virus (rather the surface protein) do not infect and replicate.
A person may be positive for surface protein antigen but he is not infectious. He will not develop cirrhosis or liver cancer.
However, a chronic hepatitis B carrier may be positive for surface protein antigen; positive for antibodies against surface protein; and positive for antibodies against hepatitis core protein. Recall that core protein contains the capsid that protects the DNA and DNA polymerase responsible for replication. That is, this person has a risk for the relapse of hepatitis B. A reason why a person with chronic hepatitis B may need an indefinite period of medication, if the medication is ineffective or weak.
A person can be a chronic hepatitis B carrier even if his viral load is less than 20,000 IU/ml. Here, viral load means that the blood contains only surface proteins. In other words, his blood does not contain DNA infectious particles. How do we know that this is so?
The person will not have a relapse of hepatitis B for a long time, assuming that he had not been reinfected by external sources. His viral load and ALT will not increase.
Drugs for hepatitis B
Drugs (lamivudine. Interferon and more) are designed to inhibit the activities of DNA polymerase thus replication of the virus. However, the virus has developed resistance against them, according to Dr. Steven-Hub Han, MD.
Chelation therapy versus hepatitis B
Just discovered last 2012, infusion chelation therapy treats hepatitis B. Dr. Arturo V. Estuita, MD discovered that when a patient with hepatitis B requested him to try this treatment on him. The patient was applying for a job in an ocean-going ship. But for his hepatitis B he could not be employed. Dr. Estuita issued a certification that his viral load was 10,000 IU/ml after treatment. The shipping company still required the applicant to go through a blood test by its accredited clinic that agreed to the certification given by Dr. Estuita. The fellow is now a crew of the ship. Since then about 20 hepatitis B patients had been treated. Their names could not be mentioned here because confidentiality is mandated for hepatitis B, like HIV.
Chelation therapy has been found as safe and effective for heart disease and diabetes by the USA Institutes for Health (Institute for Heart, Lung and Blood). A double blind randomized with control study “Trial to Assess Chelation Therapy” (TACT) was launched in 2002 that ended in March 2011. Results of TACT were presented in meeting of the American Heart Association held in Los Angeles, California in November 4,2014.( I have a Hub “USA Has Announced Chelation Therapy as Safe and Effective for Heart Disease and Diabetes”).
Chelation therapy also treats hepatitis B as discovered by Dr. Estuita who is now administering it in his clinical practice.
Chelation is an affair between the chelation solution and the hepatitis virus. Chelation solution consists of disodium EDTA (ethylene-diamine-tetra-acetate), vitamins and minerals. In the case of hepatitis B EDTA binds with and removes virus to be disposed off through the urine. It is like a crab pinching a prey with its pinchers. EDTA has six pinchers, as it were.
Hubs related to hepatitis B written by conradofontanilla
http://conradofontanilla.hubpages.com/hub/Theories-of-Hepatitis-B-as-Bases-of-Treatment
http://conradofontanilla.hubpages.com/hub/Now-A-Medical-Breakthrough-in-the-Control-of-Hepatitis-B
http://conradofontanilla.hubpages.com/hub/Treament-for-Hepatitis-B-Prevent-Hepatitis-D
http://conradofontanilla.hubpages.com/hub/Hepatitis-B-Puts-You-AT-Risk-Of-Getting-Sick-Of-Liver-Cancer-And-Cirrhosis






