Acute Rheumatic Fever: Physical Presentations And Health Significance In Multi- Organ Affection

Manifestations Of Acute Rheumatic Fever

A General Overview
Acute rheumatic fever affects multiple organs, depending on its progression and stage. The commonest organs affected are: the heart, joints, body coordination and the skin. The Health implications, pathology, causes, epidemiology and its progression as an infective disease has been discussed in the previous hub. Just go down this hub and click on the previous hub in the slide show to go through it.
In some cases, prodromal symptoms include epitasix (bleeding from the nose), erythema nodosum and vague discomfort. Rheumatic fever starts abruptly as a remittent or intermittent pyrexia with characteristic sweating. In many cases, other manifestations may not develop for considerable periods, so that the diagnosis may be unsuspected in them. In 20 to 50% of cases, the fever is accompanied by polyarthritis and carditis. Sometimes these are mild and go unrecognized especially in children.
Knee Arthritis In A Rheumatic Fever Patient

Arthritis
Acute arthritis affecting the major joints is the characteristic involvement. The joints show signs of acute inflammation and exquisite pain which make the subject immobile. Knees and ankles are most often affected followed by hips, elbows, wrists and shoulders. Small joints are affected only rarely. The arthritis is migratory and fleeting and leaves behind no residual changes. Sometimes the manifestation may be subacute with arthralgia, pain and tenderness over the neighbouring tendons and muscles. This is generally described as growing pains in children. Jaccoud’s arthritis is a rare form of rheumatic arthritis where joint deformities are more common and this resembles rheumatoid arthritis, but cardiac involvement is rare.
Radiograph Of Carditis In Rheumatic Fever
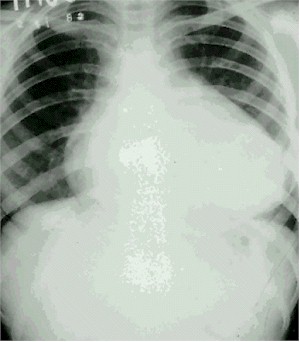
Carditis
There may be clinical features of endocarditis, myocarditis, and pericarditis in varying combinations. Tachycardia out of proportion of fever, arrhythmias, gallop rhythm, and congestive cardiac failure should suggest the presence of myocarditis. Mild cardiomegaly may be evident in the skiagrams. Arrhythmias include frequent ectopics, paroxysmal tachycardias, atrial fibrillation and heart blocks.
Presence of endocarditis is evidence by the appearance of murmurs or change in the quality of the already existing murmurs. Mitral, aortic, tricuspid and pulmonary valves are affected in the order of frequency. Actue valvulitis may lead to mitral and aortic regurgugation. Sometimes, a low pitched mid-diastolic murmur may be heard in the mitral area due to acute mitral valvulitis (Carey- Coomb’s murmur). It is transient and disappears as the valvulitis aubsides. As the valvulitis heals, fibrosis occurs and this distorts the valve apparatus resulting in stenotic and regurgitant lesions. Pericarditis is clinically manifested as chest pain, presence of pericardial rub, or a small pericardial effusion.
Sydenham’s Chorea In A Scarlet Fever Patient


Rheumatic Chores (Sydenham’s Chorea, St. Vitus Dance, Minor Chorea)
Since chorea sets in much later than the other manifestations of rheumatic fever, in many cases, it may be the only abnormality encountered. Chorea is more common in females. It is characterized by involuntary movements which are quasi-purposive, no- repititve, rapid and jerky; and these involve mainly the distal joints. Upper limbs are mostly involved, but the lower limbs, face and tongue may also be involved to a lesser extent. These movements may be mistaken for tantrums or fidgety behaviour. Emotional disturbances are frequent and these aggravate the chorea. The limbs are hypnotic and when the hands are held outstretched, they assume characteristic postures (choreic hand). The movements disappear during sleep. Chorea is self-limiting and it completely disappears withint weeks or months, without leaving any neurological sequel. Subjects developing chorea have a higher incidence of cardiac involvement.
Skin Manifestations In Scarlet Fever

Skin Manifestations
Subcutaneous nodules: They are firm, non tender, pea-sized nodules seen over the extensor aspects of the forearm, elbows, ankles, scalp and scapulae. These last for 1 to 2 weeks and disappear. The risk of carditis is high in those who develop rheumatic nodules.
Erythema marginatum: These are erythematous non- pruritic annular lesions with serpiginous borders, usually seen over the anterior aspects of the chest and abdomen and over the thighs. They spread peripherally like ripple with central clearing. The lesions blanch with pressure. In coloured races, this lesion is difficult to identify, unless carefully examined in good light.
In conclusion, other rheumatic manifestations include, pleurisy and pneumonitis which are not generally evident clinically, these are made out more often by investigations.
© 2014 Funom Theophilus Makama


