Developmental Dysplasia of the Hips (DDH)

What is DDH?
Developmental dysplasia of the hip (previously referred to as congenital dysplasia of the hip or CDH), is an abnormality of the hip joint that usually occurs at or around the time of birth, in which the femoral head is not seated deeply into the hip socket (acetabulum). There are multiple factors that contribute to this problem. First, the fetus is developing in the uterus and as the fetus grows, the space becomes progressively cramped. The hips are flexed for a long period of time, resulting in a number of changes in the hip joint. The psoas tendon which runs across the front of the joint becomes very tight and contracted. In addition, the femoral heads are only cartilage at this time. Cartilage is soft and deforms easily, so the femoral heads become egg-shaped instead of perfectly round. When the baby is born, the hips are extended and the egg-shaped femoral heads break their suction with the acetabululm, allowing the hips to slip out. The psoas acts as a lever.
The mother is secreting a hormone called relaxin which allows the ligaments around the pelvis to loosen so that the baby can come through the birth canal. This hormone also acts on the baby's ligaments, loosening the hip joints.
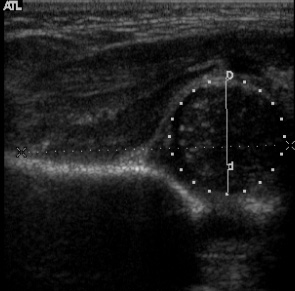
The result is that when the child is born, the hips may be completely out of the socket (dislocated), partially out of the socket (subluxated), or in the socket but easily pushed out (subluxatable).
Ultrasound of a subluxated hip
Risk Factors for DDH
The four major risk factors are: Breech position in the uterus, female, first child, and family history of DDH.
Breech presentation (in which the unborn child's bottom is facing down instead of up) may cause DDH since it increases the flexion of the hip and allows the muscles in front of the hip to be tighter. At birth, when the legs are straightened, the muscles act like a tether, forcing the hip out the back of the joint. About 30% of children that were breech will have some form of DDH. It is believed that females are more at risk because they likely have more receptors for Relaxin, the hormone secreted by the mother to loosen the ligaments in her pelvis to let the baby come out. First children are at risk because the uterus is tighter (hasn't been stretched out) and finally, there is clearly some genetic factors that increase the likelihood since DDH can run in families.
Xray of breech presentation

Signs of Hip Dysplasia
Early signs in the newborn include a shortened leg (called Galleazi's sign), asymmetric thigh folds, and a "clunk" in those hips that can be pushed in or out (Ortoloni and Barlow maneuvers). The dislocated hip or subluxated hip is not painful to the newborn child.
In older children (>3months of age), asymmetric abduction of the hip may be present. Leg length discrepancies will be noticeable in walking age children with one hip out, but if both hips are affected, there may be no difference in the leg lengths and only a wide perineum and a waddling type gait.
Asymmetric Thigh Folds
Positive Galeazzi sign

What happens if DDH is not treated?
If DDH is not treated, over time the hip can become arthritic and painful. If the hip is out completely, pain and arthritis will develop around 40 or 50 years of age. However, if the hip is subluxated (partially in), the results are worse. The hip sees very high pressures over a small surface area, wearing out the cartilage. These patients can develop pain and arthritis when they are only teenagers.
Thus early identification and treatment are important. If your pediatrician detects hip dysplasia, they will refer you to a pediatric orthopaedic surgeon for further care.
How is DDH treated?
The pediatrician will check the infant's hips multiple times after birth and in the first year of life for this problem. If he or she suspects a problem, they may order an ultrasound of the hip to document its position (x-rays generally aren't useful before 6 months of age because the hip is mostly cartilage which doesn't show up on an x-ray). If that ultrasound is positive, they should refer you to a pediatric orthopaedic surgeon for treatment.
Early treatment is generally with the Pavlik Harness, a cloth device that keeps the child's hips flexed and allows the femoral head to slip back into the acetabulum (socket). Sometimes, other braces such as the Ilfeld splint will be used if the Pavlik harness does not work.
If the problem is identified between 6 months and a year of age, an arthrogram (in which dye is injected into the joint to visualize it) and a closed reduction (in which the surgeon pushes the hip back into place and applies a body cast to hold it there) is needed. Hips that are dislocated after a year usually require an open surgery (called an "open reduction") to put the hip back in. Here, the hip joint is opened up and cleaned out. Constricting ligaments and material within the hip socket that are obstructing the head from going deeply within the socket (reduction) are removed. The capsule (thick material that surrounds the hip joint) is then repaired to keep the hip in the right place. Finally, a spica cast (body cast) is applied to help hold the hip in place.
Obviously, it is better to have the hip treated early with the Pavlik harness then to undergo these more extensive procedures, which is why the pediatrician checks your child so often.
Child in a Pavlik Harness

Follow-up
The child with DDH should be followed by a pediatric orthopaedic surgeon until maturity to be sure that the hip continues to develop normally. On occasion, the growth of the cup (the acetabulum) will not keep up, resulting in acetabular dysplasia. This again can result in early arthritic change if not treated. If the cup's roof is too vertical and/or the cup is too shallow, excessive pressure is seen by the cartilage and the hip will wear out quickly, resulting in arthritis.
What if even after treatment the hip is still abnormal?
When this occurs, surgery may be needed to cover the hip (a pelvic osteotomy). There are a number of different types, including the Salter (or innominate) osteotomy, the Triple (or Steel) osteotomy, the Ganz (or periacetabular, POA) osteotomy. All of these procedures cut the pelvis in one or more places and then the surgeon moves the roof of the acetabulum into a better position. The goal of these surgeries is to prevent arthritis and the need for a joint replacement in the future. They are complicated procedures and should be performed by a pediatric orthopaedic surgeon or a hip surgeon with significant experience in such procedures.
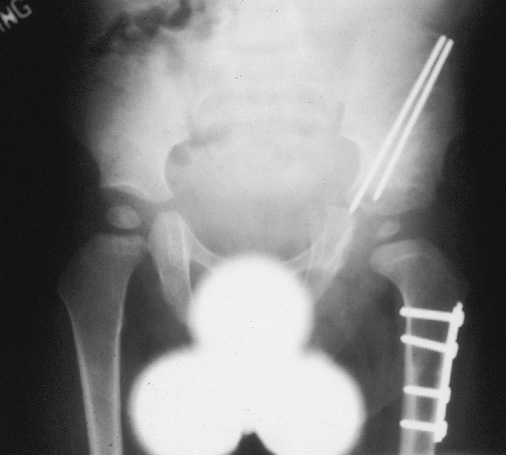
X-ray of a dislocated hip in a 2 year old

X-ray same patient after surgical correction
Other procedures
Sometimes, the hip is too shallow or injured to allow these "coverage" types of procedures. The surgeon may recommend other types of osteotomies (a Shelf or Chiari) to cover the joint and improve function temporarily, recognizing that the hip will likely need to be replaced later. These procedures cover the hip with material that is not normal joint cartilage. Because of this, they won't last the child's whole lifetime. Thus, they are considered "salvage" procedures. A salvage procedure is usually recommended when the child has too many advanced changes in the hip but is too young for a joint replacement.
Finally, if there is severe arthritic change in the hip joint, a total joint arthroplasty (total hip replacement) will be recommended. This replaces the abnormal hip joint with a metal and plastic joint. these function very well and relieve pain, but do not last a lifetime and may need to be revised with new metal and plastic in the future.
Summary
DDH or hip dysplasia is a fairly common problem, most often associated with the risk factors of breech presentation, first born, female, and a family history. If recognized and treated early, it generally results in a normal hip that does not require surgery. However, if diagnosed at a later date, surgery is much more common and may result in a poorer result.


