Pathogenesis, Clinical Manifestation And Treatment Of Infectious Mononucleosis (The Kissing Disease)

The kissing Disease

An Overview
This is worldwide in distribution, occurring in young individuals more frequently and caused by Epstein-Barr (EB) virus. It is possible that the disease may be acquired by intimate oral contact like kissing, hence its funny name, “The Kissing Disease”.
Pathogenesis
Only B lymphocytes have receptors for EB virus and therefore EB virus attacks B lymphocytes initially. These cells begin to proliferate and are altered antigenically. Though T lymphocytes are not affected by EB virus, they also proliferate enormously. Around 90% of the atypical lymphocytes which are characteristic of the disease have T lymphocyte markers, whereas only 10% have B lymphocyte markers. The T cells destroy EB virus infected B cells resulting in the liberation of antigenic materials which stimulate the formation of autoantibodies. The antigenic stimulus to heterophilic antibody is not known.
Clinical picture resembling infectious mononucleosis can be evoked by Toxoplasma gondii and cytomegalovirus, but in these, the antibody responses are not seen.
Body Hemorrhages In Infectious Mononucleosis

Clinical presentation
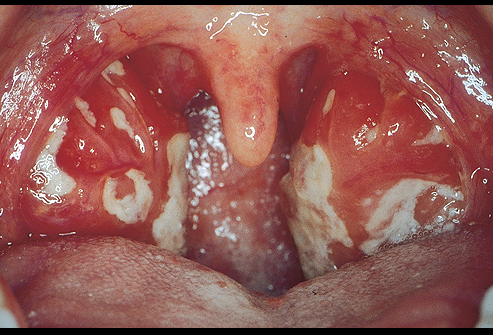
The incubation period tanges from 5- 10 days. The clinical spectrum may vary from that of a mild benign illness to that of a more severe and prolonged one. The onset is usually insidious with general malaise, headache, diffuse myalgia, variable grades of fever and other constitutional symptoms. A petechial rash occurring at the junction of the soft and hard palate associated with sore throat may herald the onset. The sore throat may persist for days and this may be mistaken for follicular tonsillitis. The posterior cervical lymph nodes enlarge initially, later, generalized lymphadenopathy may occur.
Spleen is moderately enlarged to 2 to 3 cm below the costal margin, it is soft and not tender. If gross splenomegaly occurs, the organ tends to rupture even with slight trauma. Rarely jaundice and neurological manifestations may develop.
Blood
Initially, there is leucopenia due to decrease in neutrophils. But this is followed by leucocytosis in which the leucocyte count may go up to 15- 20,000/cmm. The characteristic finding is the presence of atypical lymphocytes which may form 60-80% of the total. The nuclei of the atypical lymphocytes do not have a regular shape but may be kidney shaped, oval, lobulated or polymorphic. Nucleoli are not seen. The cytoplasm is non granular, foamy, vacuolated and appears amoeboid. In uncomplicated cases, platelet count is normal.
Symptomatology

Diagnosis And Treatment
Clinically, the disease should be suspected when small outbreaks occur in closed communities like hostels and dormitories, or when there is a close personal contact with cases. The presence of oral lesions, posterior cervical lymphadenopathy, splenomegaly and erythematous rashes are suggestive. Diagnosis should be strongly suspected if the proportion of atypical lymphocytes exceed 50%.
Presence of heterophilic antibodies demonstrable by the Paul-Bunnell test (Sheep-cell agglutination) strongly suggests the diagnosis of infectious mononucleosis. The titer of antibodies increases with the passage of time. They are detectable for 4 to 6 weeks. Since similar antibodies develop in serum-sickness as well, differential infectious mononucleosis antibodies from those due to serum sickness.
Recently a rapid slide test called “mono test” has become available for quick diagnosis. Specific antibody to EB virus can be demonstrated by immunofluorescence. Complement fixation and gel diffusion wherever facilities exist.
The differential diagnosis includes rubella, measles, viral hepatitis, secondary syphilis, follicular tonsillitis, diphtheria and herpetic pharyngitis. The prolonged fever and constitutional symptoms may suggest enteric fever. Influenza, or even acute rheumatic fever. The cases which present with neurological manifestations may have to be distinguished from encephalitis or lymphocytic choriomeningitis. Other hematological disorders like acute leukemia and lymphoma have to be distinguished by suitable tests.
Treatment
There is no specific therapy and symptomatic measures are indicated. It is seen that ampicillin aggravates the lymphadenopathy, skin rash and laryngeal edema in many cases and hence this drug should not be employed. Antibodies are indicated if there is evidence of secondary infection. In severe cases, corticosteroids may help, especially when there is respiratory distress. In the vast majority, recovery is usually complete in 3- 4weeks without any sequelae. Recent epidemiological evidence suggests that in some cases, due to continued antigenic stimulation, a lymphomatous process may be triggered off.
© 2014 Funom Theophilus Makama


: Symptoms, Causes, and Treatments")



