Special Types Of Anemia: Sideroblastic Anemias And Paroxysmal Nocturnal Hemoglobinuria (PNH)

Symptomatology Of Sideroblastic Anemia

Sideroblastic Anemias
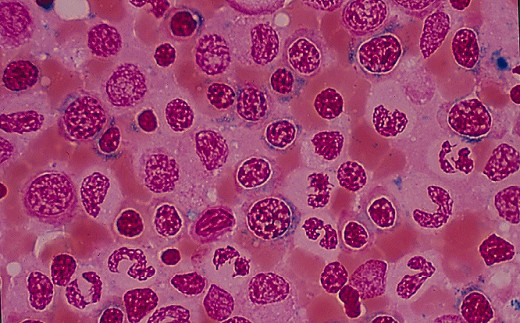
Anemias may result from impaired red cell production due to disorder in the synthesis of heme. The term sideroblast denotes an erythroblast containing one or two stainable Iron granules in the cytoplasm. When such stainable Iron granules are present in the erythrocyte, it is called siderocyte. Even under normal conditions, a few of these Iron granules may be seen lying free in the cytoplasm without relation to any particular organelle within the cell. But under pathological conditions, Iron granules accumulate in the mitochondria and they appear in the form of a perinuclear ring in the late erythroblasts and such cells are called ringed sideroblasts. Sometimes, pathological non-ringed sideroblasts occur, with excess of free Iron granules in the cytoplasm.
Sideroblastic Anemia In Blood Smear
Etiology
Sideroblastic anemia may be hereditary or acquired. The hereditary form shows a sex-lined inheritance, manifesting in males and being transmitted by females. It manifests as a microcytic hypochromic anemia resistant to Iron therapy. It follows a benign course.
The acquired form is seen in elderly subjects. In the majority of cases there is no detectable cause but known causes include rheumatoid disease, malignancy, myelosclerosis, chronic myeloid and lymphatic leukemias, acute leukemia, myeloma, polycythemia vera, myxedema, pyridoxine deficiency (nutritional and that induced by antituberculous drugs like INH), alcoholism, lead poisoning, ingestion of drugs like chloramphenicol, cycloserin and rifampicin and erythrocytic porphyria.
Diagnosis should be suspected when a patient with microcytic hypochromic anemia fails to respond to adequate Iron therapy. Diagnosis is established by the demonstration of ringed sideroblasts in the bone marrow stained for Iron by Prussian blue reaction.

Prognosis And Treatment
Course and prognosis
In secondary cases, prompt clinical improvement occurs on removal of the primary cause. The idiopathic fomr may be resistant to all forms of therapy. Some cases of idiopathic sideroblastic anemia progress to acute myeloid leukemia and, therefore, this may be considered as one of the preleukemia conditions.
Treatment
The primary cause, if identified, should be rectified. In the presence of overt pyridoxine deficiency, small doses of pyridoxine (5-10 mg) are effective. Rarely even in the idiopathic variety, large doses of pyridoxine given orally (100-500 mg/daily) are beneficial and, therefore, this should be given a trial. Concomittant folate deficiency should be corrected by oral folic acid 5 mg/day. In resistant cases, symptomatic relief can be achieved with regular transfusion of packed erythrocytes.
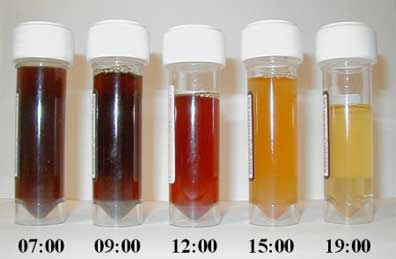
Laboratory Findings Of Paroxysmal Nocturnal Hemoglobinuria
Symptomatology

Paroxysmal Nocturnal Hemoglobinuria
This is a rare acquired chronic hemolytic disorder affecting both sexes usually in the middle age. The name is derived from the fact that intravascular hemolysis and hemoglobinuria occur more frequently in the morning intermittently. In addition to hemoglobin, hemosiderin is also present in urine. This disease is considered to be an acquired erythrocyte stem cell disorder where a clone of abnormal erythrocytes proliferates. The erythrocyte membrane is defective. The erythrocytes undergo auto-hemolysis through the complement-mediated pathway with consequent reduction in complement levels. The condition presents as chronic anemia with or without jaundice and splenomegaly. Hemoglobinuria may be precipitated by drugs. Infections or transfusion of whole blood. Complications may occur rarely. These are thrombosis of portal venous system, aplastic crises, and Iron deficiency due to urinary loss of Iron. The traction of hemosiderin in the urinary deposits by Prussian blue reaction. Diagnosis is confirmed by the Ham test and sucrose lysis test, both of which demonstrate abnormal lysis of red cells in acid pH or sucrose solution respectively.
The treatment is supportive as no drug is available to control hemolysis. Severe anemia should be treated by transfusion of washed erythrocytes, since introduction of fresh complement in transfused plasma may provoke a fresh bout of hemolysis.
© 2014 Funom Theophilus Makama




