The Pathology, Causes Clinical Manifestations And The Complete Course Of Treatment Of Polycythemia

Polycythemia Vera

A General Overview
Though, the term polycythemia actually signifies increase in the number of all formed elements of blood, usually, it is used to describe an increase in erythrocytes. Polycythemia may be absolute when the number of cells is actually increased or relative when the plasma volume is decreased, without actual increase in cells.
Causes Of Polycythemia
A. TRUE POLYCYTHEMIA
| |
|---|---|
I. Polycythemia rubra vera
| |
II. Secondary polycythermia
| |
1. High altitude
| |
2. Cyanotic congenital heart disease
| |
3. Chronic lung disease with alveolar hypoventilation
| (Points 1 to 6)- Lowering of arterial oxygen tension stimuaties erythropoietin production as a compensatory mechanism
|
4. Hemoglobinopathies which interfere with oxygen dissociation in the tissues and methemoglobinemia
| |
5. Obesity with Pickwickian syndrome
| |
6. Heavy smoking
| |
7. Renal carcinoma and other lesions like hydronephrosis and polycystic kidneys
| (Points 7 to 9)- increased or inappropriate erythropoietin production leads to polycythemia
|
8. Carcinoma liver, unterine fibromyomas, cerebellar hemangioblastomas
| |
9. Endocrine abnormalities like Cushing’s syndrome and pheochromocytoma
| |
10. Drugs like corticosteroids, anabolic steroids, cobalt salts etc
| |
B. RELATIVE POLYCYTHEMIA
| |
Dehydration and loss of plasma as in burns and polycythemia of stress (pseudopolycythemia)
| Erythropoietin levels are normal
|
Polycythemia In Blood Sample
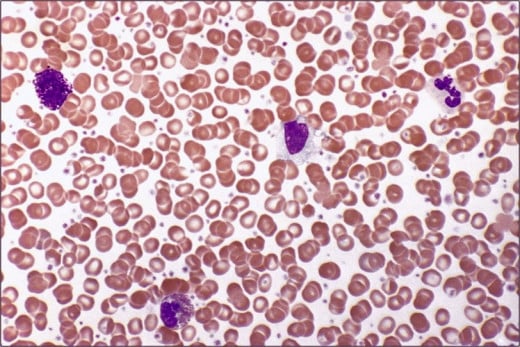
Polycythemia Rubra Vera (Erythremia)
Also known as Vasquez’a disease, Osler’s or cryptogenic polycythemia. This is a chronic progressive disorder which is accompanied by increase in number of all the formed elements, especially erythrocytes. The marrow is hyperplastic. Polycythemia vera is considered to be a benign neoplastic proliferation of the marrow. Plasma erythropoietin levels are normal or low.
Pathology
There is increase in total red cell volume above 36 ml/Kg in men and 32 ml/Kg in women. The cellular volume increases disproportionately with only less degrees of increase of plasma volume. The net result is a gross increase in blood volume. The rise in granulocytes and platelets is less marked though they are also increased. The usual indices for diagnosis are:
- Hemoglobin above 17.5 g/dl in males and 15.5 g/dl in females.
- The red cell count above 6 X 1012/liter in males and 5.5 X 1012/liter in females, and
- Hematocrit above 55% in males and 47% in females.
The high viscosity of the blood leads to sludging in small vessels and thrombosis and occlusion of the microcirculation of vital organs. Hemorrhages occur at times. This is due to damage to the capillaries and also dysfunction of the platelets. Hyperuricemia occurs due to increased cell turn over.
Cyanosis In Polycythemia


Clinical Manifestations
Diagnosis of Polycythemias
Clinically, the diagnosis should be suggested by the ruddy cyanosis, injected eyes, mild splenomegaly, and the blood counts.
The disease has to be distinguished from early phase of CML and myelofibrosis. In all cases, full investigations should be undertaken to detect an underlying cause. Among the common underlying causes, renal carcinoma, congenital cyanotic heart disease and chronic respiratory disease top the list.
Course and prognosis of polycythemias
Half of the subjects die within 18 months of the onset due to thrombotic complications, development of acute leukemia (15%), or myelofibrosis (30%). Treatment improves the lifespan. Patients treated with simple repeated venesection have a median survival of 4-5 years and in those treated with radiotherapy, it may increase to 10-15 years
Complications of polycythemias
Hemorrhages and vascular occlusions are not uncommon. Polycythemia may transform into acute myeloid leukemia, myelofibrosis, or chronic myeloid leukemia on prolonged follow up. Other complications include cardiac failure, hypertension and secondary gout.
Venesection

Cytotoxic Drugs
Treatment of polycythemias
Therapy aims at keeping the blood volume normal with the PCV around 40-45%.
Venesection: This is the simplest and most effective method to reduce blood volume. A quantity of 500 ml of blood is withdrawn on alternate days to bring down the blood volume to normal. This blood can be useful for further transfusion. Usually, the blood volume is normalized by venesection 4-6 times. There after, the interval between phlebotomies is increased. Since the blood is thick and shows a high tendency to clot, a large bore needle is required. With venesection, only the red cell count comes down. Ultimately, Iron deficiency state develops. Mild degrees of Iron deficiency may help to depress erythropoiesis, but if this is severe, Iron therapy is required.
Radioactive Phosphorus (32P): This is a beta emitter isotope. When administered, it is concentrated in the bone and the marrow is irradiated. Initial dose is 3-5 millicuries given intravenously. This dose can be repeated after 2-3 months, if necessary. Remission induced by a dose of 32P treatment is contraindicated during pregnancy.
Cytotoxic drugs: Drugs like busulfan 2- 4 mg/day, cyclophosphamide 2 mg/Kg and chlorambucil 2- 5 mg/Kg bring about remission in 80% of cases if given continuously for weeks. Pyrimethamine (Daraprim) which is an antimalarial, in a dose of 25- 100 mg, a day is beneficial, but this may lead to megaloblastic anemia. This side effect should be watched for, it responds to folic acid.
© 2014 Funom Theophilus Makama
Related

Stasis Dermatitis - Pictures, Symptoms, Causes, Treatment, Diagnosis

Aplastic Anaemia: A Rare and Serious Blood Disorder Targeting Youths?

Clinical Manifestations Of Hypothyroidism: Cretinism, Myxedema, Hoffman’s Syndrome And Pendred’s Syndrome

Differences between Hemophilia and Thalassemia

Enlarged Aorta - Symptoms, Treatment, Surgery, Pictures


