SNHU: Abnormal Psychology: Clinical Perspectives on Psychological Disorders Chapter 3 Notes

Chapter 3: Assessment
- Case Report: Ben Robsham
- Reason for referral: Ben is a 22-year-old Caucasian male with 12 years of formal education who was referred to the clinic by his supervisor following an incident in which he hit his head while operating a subway train. While driving above ground, Ben reported that the brakes had jammed while he was coming to an intersection where pedestrians were crossing. Using the emergency brake, Ben was able to stop the train, but the abrupt halt caused him to hit his head on the glass window and temporarily lose consciousness. He is unable to recall what happened directly after hitting his head. Ben took a two-week leave of absence after the incident, and continued to avoid going to work for the two following weeks. When the supervisor called him, Ben stated, “I can't leave my house. They'll come and get me.”
- Relevant history: Ben has no history of psychiatric treatment. He stated that he has never experienced depression or anxiety, and that he typically feels “just fine,” which has made the recent changes in his psychological state all the more disturbing to him. Ben reported that he has never used drugs and only occasionally drinks when he is in a social environment. Additionally, Ben reported that his maternal grandfather and uncle had both been diagnosed with schizophrenia. Finally, Ben reported having no remarkable past or current medical history.
- Case formulation: Because Ben's symptoms emerged following the incident; Ben will be referred for neuropsychological testing to rule out possible traumatic brain injury.
- Diagnosis: Rule out mild neurocognitive disorder due to traumatic brain injury with behavioral disturbance.
- Treatment plan: After an initial intake interview at the university, Ben was referred for further psychological evaluation and psychiatric consultation to Dr. Martin Washington, a neuropsychologist.
- Tests administered
- Clinical Interview
- Wechsler Adult Intelligence Scale, Fourth Edition (WAIS-IV)
- Trail-Making Test, Parts A and B
- Clock Drawing Test
- Paced Auditory Serial Addition Test (PASAT)
- Boston Naming Test, Second Edition (BNT)
- Wechsler Memory Scale (WMS)
- Minnesota Multiphasic Personality Inventory-2 (MMPI-2)
- 3.1: Characteristics of Psychological Assessments
- A psychological assessment is a procedure in which a clinician provides a formal evaluation of an individual's cognitive, personality, and psychosocial functioning.
- Clinicians conduct assessments under a variety of conditions. In many cases, clinicians use the assessment process to provide a diagnosis, or at least a tentative diagnosis, of an individual's psychological disorder. However, clinicians may also use assessments for a variety of other reasons.
- Ex. - In forensic assessments, clinicians determine whether a suspect meets the criteria of being competent to stand trial.
- Clinicians might also provide information that employers can use to evaluate an individual's appropriateness for a particular job. Assessments are also useful when clinicians consult about an individual's level of functioning in a specific area.
- Ex. - An older woman experiencing memory problems may seek neuropsychological assessment to determine whether she has a cognitive impairment that will require further intervention.
- To be useful, clinicians must hold assessments to standards that ensure that they provide the most reproducible and accurate results. The reliability of a test indicates the consistency of the scores it produces.
- In other words, it should produce the same results regardless of when it is given, and the individual should answer test items in similar fashion. The test's validity reflects the extent to which a test measures what it is designed to measure. An intelligence test should measure intelligence, not personality. Before using a given test, clinicians should be aware of its reliability and validity, information that is readily available in the published literature about the instrument.
- The profession strives to design tests so that the results they produce don't vary from clinician to clinician. The criterion of standardization clearly specifies a test's instructions for administration and scoring. Each individual receiving the test should have the same amount of time, and each person scoring the test should do so in the same manner according to the same, predefined criteria.
- In addition to determining a test's reliability and validity, it is important to take into account its applicability to test-takers from a diversity of backgrounds. Increasingly, test publishers are designing their measures for usage with a variety of individuals in terms of ability level, first language, cultural background, and age. For example, clinicians may need to adapt assessment instruments for use with older adults, who may require larger print, slower timing, or special writing instruments for use with those who have arthritis.
- When interpreting test results, clinicians need to ensure that they don't fall into the trap of the so-called “Barnum Effect.” Named after legendary circus owner P. T. Barnum, this is the tendency for clinicians unintentionally to make generic and vague statements about their clients that do not specifically characterize the client.
- Ex. - of a Barnum Effect statement: “Julia is often shy around other people, but at times she can be very outgoing. When presented with a challenge, she can often perform very well, but she occasionally becomes nervous and intimidated.”
- These two sentences could apply to Julia, but they could also apply to most other people. Therefore, they don't say anything special about Julia. Furthermore, most people would find it difficult to disagree with this feedback.
- In a clinical situation, the problem is that such statements are not particularly insightful or revealing and do not help inform the assessment process.
- Clinicians should keep up with the literature to ensure that they are using the best assessment methods possible. Evidence-based assessment includes (1) relying on research findings and scientifically viable theories; (2) using psychometrically strong measures; and (3) empirically evaluating the assessment process. By following these guidelines, clinicians ensure that they will evaluate their clients using the most current and appropriate materials available.
- Ex. - A seasoned clinician may have a preference for using the assessment methods she learned about in graduate school, but she should be constantly alert for newer procedures that rely on newer technology or research.
- According to criterion (3), she should also develop evaluation methods to assess whether her assessments are providing useful information about her clients.
- Ex. - Consider the case of an assessment suggesting that a client is experiencing significant depressive symptoms even though she seeks help for what she describes as attacks of anxiety. Following the criteria for evidence-based assessment, the clinician would determine whether the tool or tools she used to make the diagnosis provided an accurate characterization of the woman's symptoms as they evolved over the course of treatment.
- Similarly, in Ben's case, the clinician must validate the findings from neuropsychological assessment carefully by obtaining multiple measures to assess possible brain injury.
- Ex. - A seasoned clinician may have a preference for using the assessment methods she learned about in graduate school, but she should be constantly alert for newer procedures that rely on newer technology or research.
- 3.2: Clinical Interview
- Clinicians typically begin their assessment with the clinical interview, a series of questions that they administer in face-to-face interaction with the client.
- The answers the client gives to these questions provide important background information on clients, allow them to describe their symptoms, and enable clinicians to make observations of their clients that can guide decisions about the next steps, which may include further testing.
- The least formal version of the clinical interview is the unstructured interview, which consists of a series of open-ended questions regarding the client's symptoms, health status, family background, life history, and reasons for seeking help. In addition to noting the answers to these questions, the clinician also observes the client's body language.
- By noting the client's nonverbal cues, the clinician can gain an understanding of whether the client is experiencing anxiety, attentional difficulties, unwillingness to cooperate, or unusual concern about testing. The clinician may also use cues from the client's appearance that give further indication of the client's symptoms, emotional state, or interpersonal difficulties.
- Clinicians typically begin their assessment with the clinical interview, a series of questions that they administer in face-to-face interaction with the client.
Topic
| Purpose
|
|---|---|
Age and sex
| Obtain basic demographic information.
|
Reason for referral
| Hear client's reason for seeking treatment, in his or her own words.
|
Education and work history
| Obtain socioeconomic status and determine whether client is still working.
|
Current social situation
| Find out whether client is currently in a relationship and how much social support is potentially available.
|
Physical and mental health history
| Determine whether client has any medical illnesses and whether there has been a recent change in health.
|
Find out about history of present problem including past diagnoses and treatments and whether treatment was helpful or not.
| |
Drug/alcohol use and current medication
| Ascertain whether client is using psychoactive drugs (including alcohol and caffeine). Obtain list of medications to avoid potential interactions with any psychopharmacological interventions.
|
Family history
| Find out whether client's family has medical and psychological disorders, particularly any relevant to client's current symptoms.
|
Behavioral observations
| Note behaviors, including nonverbal behaviors, which indicate whether client is experiencing anxiety or altered mood. Also note whether client seems to be experiencing difficulties in attention or compliance. Attempt to determine client's mental status. Compare client's appearance with stated age. Determine whether client is oriented to time, place, and person. Observe any unusual motor behaviors.
|
- The clinical interview is a key step in the diagnostic process because of the information it provides regarding the client's current symptoms, history, and availability of social support. Over the course of a 30- to 45-minute interview, the clinician must help the client feel as relaxed as possible. Because the client is providing highly personal information, the clinician attempts to draw the client out with questioning that is respectful, but also matter-of-fact. The clinical interview is not like an ordinary conversation in that respect.
- Unlike the clinical interview, the structured interview provides standardized questions that are worded the same way for all clients. A structured interview can either provide a diagnosis on which to further base treatment or classify the client's symptoms into a DSM disorder.
- One of the most widely used clinical interviews is the Structured Clinical Interview for DSM-IV Disorders (SCID). Though the title uses the word “Structured,” clinicians who administer the SCID modify the wording and order of questions to accommodate the particular individual whom they are examining. Clinicians use the SCID-I to make Axis I diagnoses and the SCID-II to make Axis II diagnoses. Both SCIDs are designed so that the clinician can adapt to the interviewee's particular answers. The questions are worded in standard form, but the interviewer chooses which questions to ask based on the client's answers to previous questions.
- Ex. - if a client states that she experiences symptoms of anxiety, the interviewer would follow up with specific questions about these symptoms. The interviewer would only ask follow-up questions if the client stated that she was experiencing anxiety symptoms. If she stated that she had different symptoms, such as depressed mood, then the follow-up questions would inquire further about her mood (First & Gibbon, 2004). The SCID-I takes 45 to 90 minutes to administer, depending on the complexity of the client's symptoms.

- An advantage of a structured interview is that it is a systematic approach that is less subject to variations from clinician to clinician than an unstructured interview. Furthermore, anyone with the proper training can administer the SCID, not necessarily just licensed mental health professionals. This has practical value in that clients can receive initial screening prior to their beginning a course of therapy. Furthermore, there is a research version of the SCID that professionals can use to provide systematic diagnostic information across different investigations. Researchers can feel confident that an SCID-based diagnosis of a mood disorder means the same thing regardless of who conducted the study. A SCID for DSM-5 is currently under development.
- 3.3: Mental Status Examination
- A clinician uses a mental status examination to assess a client's current state of mind. In conducting a mental status examination, the clinician assesses a number of features of the client including appearance, attitudes, behavior, mood and affect, speech, thought processes, content of thought, perception, cognition, insight, and judgment.
- The outcome of the mental status examination is a comprehensive description of how the client looks, thinks, feels, and behaves
- A clinician uses a mental status examination to assess a client's current state of mind. In conducting a mental status examination, the clinician assesses a number of features of the client including appearance, attitudes, behavior, mood and affect, speech, thought processes, content of thought, perception, cognition, insight, and judgment.
- The Mini-Mental State Examination (MMSE) is a structured tool that clinicians use as a brief screening device to assess dementia. The clinician administers a set of short memory tasks and compares the client's scores to established norms.
- If the client scores below a certain cutoff, the clinician then can (and should) continue to more in-depth testing of potential cognitive impairments.
- 3.4: Intelligence Testing
- Many professions (i.e., mental health, academia, business, government agencies) use intelligence (IQ) tests for a variety of assessments, including overall cognitive evaluation, diagnosis of learning disabilities, determination of giftedness or mental retardation, and prediction of future academic achievement. Clinicians also sometimes use IQ tests in the diagnosis of neurological and psychiatric disorders, in which cases they are a component of a more comprehensive assessment procedure. Finally, human resource departments often use IQ tests in personnel selection to evaluate the potential for employees to perform in specific conditions.
- Stanford-Binet Intelligence Test
- First developed in the early 1900s by Alfred Binet, the Stanford-Binet is now in its fifth edition, known as the Stanford-Binet 5 (SB5).
- Children taking this test receive a deviation intelligence (IQ) score, calculated by converting their raw scores to standardized scores that reflect where a child stands in relation to others of similar age and gender.
- Deviation intelligence (IQ) score - An index of intelligence derived from comparing the individual's score on an intelligence test with the mean score for that individual's reference group.
- The average deviation IQ score is set at 100 with a standard deviation of 15. If a child receives an SB5 IQ score of 115, this means that the child stands at above the IQ of 68 percent of the population.
Scale
| Definition
| Example
|
|---|---|---|
Fluid Reasoning
| Ability to solve novel problems
| Sort picture chips into groups of three
|
Knowledge
| Accumulated fund of general information
| Show how to perform a given action
|
Quantitative Reasoning
| Ability to solve problems with numbers or numerical concepts
| Count a set of items
|
Visual-Spatial Reasoning
| Ability to analyze spatial relationships and geometric concepts
| Assemble puzzle-like forms
|
Working Memory
| Ability to store, transform, and retrieve information in short-term memory
| Recall a sequence of taps
|
- Wechsler Intelligence Scales
- The first comprehensive individual test that researchers specifically designed to measure adult intelligence was the Wechsler Adult Intelligence Scale (WAIS).
Scale
| Tests
| Type of Item
|
|---|---|---|
Verbal Comprehension
| Vocabulary Information Comprehension Similarities
| Define the word “barrel” How many minutes are there in an hour? Why do plants need water? How are an elephant and a cat alike?
|
Perceptual Reasoning
| Matrix reasoning Visual puzzles Block design Picture completion
| Choose which pattern logically follows after a set of patterns Arrange a set of blocks so that they reproduce a design State what is missing in a picture of a common object
|
Working Memory
| Digit span forward Digit span backward Letter-number sequencing
| Recall a series of digits in forward order Recall a series of digits in backward order Recall a set of digits from smallest to largest Recall a set of mixed letters and numbers from largest to smallest
|
Processing Speed
| Symbol search Coding
| Copy numbers that match symbols into appropriate boxes
|
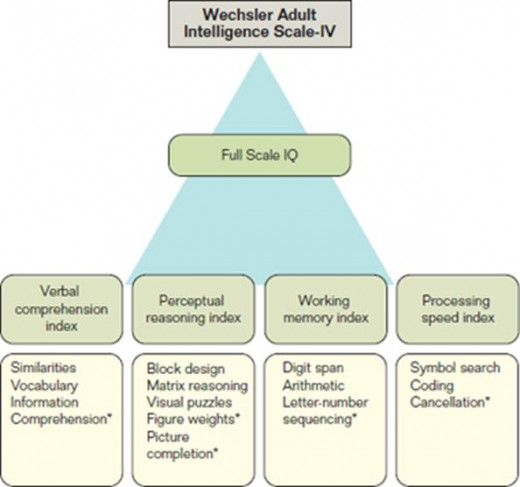
- Because the WAIS-IV is given on an individual basis, clinicians have ample opportunities to observe the test-taker's behavior during the test, possibly gaining valuable diagnostic information to complement the test scores. In fact, the instructions for the WAIS-IV scoring include suggestions for the examiner to include behavioral observations such as the individual's fluency in English; physical appearance; problems with vision, hearing, or motor behavior; difficulties with attention and concentration; motivation for testing; and any unusual behaviors that the test-taker shows.
- 3.5: Personality Testing
- Clinicians use tests of personality to understand a person's thoughts, behaviors, and emotions. There are two main forms of personality tests: self-report and projective.
- A self-report clinical inventory contains standardized questions with fixed response categories that the test-taker completes independently either on paper or on the computer. Test-takers rate the appropriateness of the item to themselves on a fixed scale. These tests are objective in the sense that the scoring does not involve any form of subjective judgment on the part of the examiner. In fact, computers can both score these tests and produce brief explanatory reports. However, clinicians need to balance the advantages of their objectivity against the possibility that these reports are subject to the Barnum Effect. Because computer programs rely on a set of algorithms to produce their reports, they run the risk of being overly generic and not tapered to the particular test-taker's idiosyncrasies.
- a major advantage of self-report inventories is that they are relatively easy to administer and score. Consequently, large numbers of people can take these in an efficient manner. Clinicians can take advantage of the wealth of information on the validity and reliability of the better-known self-report inventories when interpreting the scores of their own clients.
Clinical scales
Scale
| Scale Name
| Type of Content
| Adapted Item
|
|---|---|---|---|
1
| Hypochondriasis
| Bodily preoccupations and concerns, fear of illness and disease.
| I have a hard time with nausea and vomiting.
|
2
| Depression
| Unhappiness and feelings of low personal worth.
| I wish I were as happy as others appear to be.
|
3
| Hysteria
| Denial of psychological problems and over-reactions to stressful situations, various bodily complaints.
| Frequently my head seems to hurt everywhere.
|
4
| Psychopathic deviate
| Antisocial tendencies and delinquency.
| I was occasionally sent to the principal's office for bad behavior.
|
5
| Masculinity-femininity
| Adoption of stereotypic sex-role behaviors and attitudes.
| I like reading romantic tales (female item).
|
6
| Paranoia
| Feelings of persecution and suspiciousness of others.
| I would have been a lot more successful had others not been vindictive toward me.
|
7
| Psychasthenia
| Uncontrollable urges to think and act; unreasonable fears.
| Sometimes I think thoughts too awful to discuss.
|
8
| Schizophrenia
| Disturbances of thinking, mood, and behavior.
| I have had some rather bizarre experiences.
|
9
| Hypomania
| Elevated mood, accelerated speech and motor activity.
| I become excited at least once a week.
|
10
| Social introversion
| Tendency to withdraw from social situations.
| I usually do not speak first. I wait for others to speak to me.
|
Validity scales (composed of items from clinical scales)
Scale
| Scale Name
| Type of Content
|
|---|---|---|
L
| Lie scale
| Unrealistically positive self-representation
|
K
| Correction
| Similar to L scale—more sophisticated indication of tendency toward positive self-presentation
|
F
| Infrequency
| Presenting oneself in an unrealistically negative light
|
Scale
| Scale Name
| Type of COntent
|
|---|---|---|
RCd
| Demoralization
| General unhappiness and dissatisfaction
|
RC1
| Somatic complaints
| Diffuse physical health complaints
|
RC2
| Low positive emotions
| Lack of positive emotional responsiveness
|
RC3
| Cynicism
| Non self-referential beliefs expressing
|
RC4
| Antisocial behavior
| Rule breaking and irresponsible behavior
|
RC6
| Ideas of persecution
| Belief that others pose a threat to the self
|
RC7
| Dysfunctional negative emotions
| Maladaptive anxiety, anger, and irritability
|
RC8
| Aberrant experiences
| Unusual thoughts or perceptions
|
RC9
| Hypomanic activation
| Over-activation, aggression, impulsivity, and grandiosity
|
- A projective test is a technique in which the examiner asks the test-taker questions about an ambiguous item. The underlying idea behind projective tests is that people cannot or will not provide accurate statements on self-report inventories.
- Ex. - clients may not wish to say that they are experiencing unusual symptoms or have qualities that they deem negative. On projective tests, clients may be less guarded about their responses because they don't know how the assessor will interpret their answers. Projective tests are most useful when combined with self-report inventories rather than used as the sole basis for diagnosing or evaluating a client.
- The most famous projective technique is the Rorschach Inkblot Test, named after Swiss psychiatrist Hermann Rorschach, who developed the method in 1911. To administer the test, the examiner shows the test-taker a set of 10 cards (5 black and white, 5 with color), one by one. The test-taker's job is to describe what the inkblot looks like. Although the method sounds simple enough, over the last century researchers and clinicians continue to refine the scoring methods.
- 3.6: Behavioral Assessment
- Unlike psychological tests, behavioral assessments record actions rather than responses to rating scales or questions. The target behavior is what the client and clinician wish to change. Behavioral assessments include descriptions of the events that precede or follow the behaviors. We call events that precede the behavior antecedents and events following the behavior consequences.
- Ex. - For example, a child in a classroom may be unusually disruptive immediately following recess, but not immediately following lunch. When clinicians record behavior in its natural context, such as the classroom or the home, this is called in vivo observation. However, it's not always possible or practical to conduct an in vivo observation. The teacher or a teacher's aide is most likely too busy to record the behavior of one child, and having a clinician in the room would create a distraction or influence the behavior he or she is observing.
- Unlike psychological tests, behavioral assessments record actions rather than responses to rating scales or questions. The target behavior is what the client and clinician wish to change. Behavioral assessments include descriptions of the events that precede or follow the behaviors. We call events that precede the behavior antecedents and events following the behavior consequences.
- Analog observations take place in a setting or context such as a clinician's office or a laboratory specifically designed for observing the target behavior. A clinician assessing the disruptive child would need to arrange a situation as comparable as possible to the natural setting of the classroom for the analog observation to be useful.
- Clients may also report on their own behavior rather than having someone observe them. In a behavioral self-report the client records the target behavior, including the antecedents and consequences of the behavior.
- Self-monitoring is a form of behavioral self-report in which the client keeps a record of the frequency of specified behaviors, such as the number of cigarettes he or she smoked or calories he or she consumed, or the number of times in a day that a particular unwanted thought comes to the client's mind.
- Clinicians may also obtain information from their clients using behavioral interviewing in which they ask questions about the target behavior's frequency, antecedents, and consequences
- 3.7: Multicultural Assessment
- When psychologists conduct an assessment, they must take into account the person's cultural, ethnic, and racial background, performing a multicultural assessment.
- Clinicians evaluating clients who speak English as a second language, or do not speak English at all, must ask a number of questions: Does the client understand the assessment process sufficiently to provide informed consent? Does the client understand the instructions for the instrument? Are there normative data for the client's ethnic group? Even if clients appear as fairly fluent, they may not understand idiomatic phrases for which there are multiple meanings (Weiner & Greene, 2008).
- 3.8: Neuropsychological Assessment
- Neuropsychological assessment is the process of gathering information about a client's brain functioning on the basis of performance on psychological tests.
- Clinicians use neuropsychological assessment measures to attempt to determine the functional correlates of brain damage by comparing a client's performance on a particular test with normative data from individuals who are known to have certain types of injuries or disorders.
- There is no one set procedure for conducting a neuropsychological assessment. Particular clinicians may have preferences for certain tests, but these preferences are not set in stone.
- Moreover, neuropsychologists typically choose tests that will help them understand the client's presenting symptoms and possible diagnoses. The client's age is another factor that the clinician takes into account.
- Tests appropriate for older adults are not necessarily either appropriate or useful for diagnosing a child or adolescent.
- When psychologists conduct an assessment, they must take into account the person's cultural, ethnic, and racial background, performing a multicultural assessment.
- In a neuropsychological assessment, the clinician can choose from tests that measure attention and working (short-term) memory, processing speed, verbal reasoning and comprehension, visual reasoning, verbal memory, and visual memory. A number of tests evaluate what clinicians call “executive function,” the ability to formulate goals, make plans, carry out those plans, and then complete the plans in an effective way. There are a variety of available tests within each category. If a clinician wishes to investigate one area in depth for a particular client, then he or she will administer more tests from that category.
- 3.9: Neuroimaging
- Neuroimaging provides a picture of the brain's structures or level of activity and therefore is a useful tool for “looking” at the brain.
- The electroencephalogram (EEG) measures electrical activity in the brain. EEG activity reflects the extent to which an individual is alert, resting, sleeping, or dreaming. The EEG pattern also shows particular patterns of brain waves when an individual engages in particular mental tasks. Clinicians use EEGs to evaluate clients for conditions such as epilepsy, sleep disorders, and brain tumors.
- Computed axial tomography (CAT or CT scan) is an imaging method that clinicians and researchers use to provide an image of a cross-sectional slice of the brain from any angle or level. CT scans provide an image of the fluid-filled areas of the brain, the ventricles. The method is useful when clinicians are looking for structural damage to the brain.
- Magnetic resonance imaging (MRI) uses radio waves rather than X-rays to construct a picture of the living brain based on the water content of various tissues.
- The person is placed inside a device that contains a powerful electromagnet. This causes the nuclei in hydrogen atoms to transmit electromagnetic energy (hence the term magnetic resonance), and activity from thousands of angles is sent to a computer, which produces a high-resolution picture of the scanned area.
- The picture from the MRI differentiates areas of white matter (nerve fibers) from gray matter (nerve cells) and is useful for diagnosing diseases that affect the nerve fibers that make up the white matter. However, like the CAT scan, the MRI produces static images so it cannot monitor brain activity.
- Positron emission tomography (PET) scan, or a variant known as single photon emission computed tomography (SPECT), does provide images of brain activity. Specialists inject radioactively labeled compounds into a person's veins in very small amounts. The compounds travel through the blood into the brain and emit positively charged electrons called positrons, which they can detect much like X-rays in a CT.
- Proton magnetic resonance spectroscopy (MRS) is another scanning method that measures metabolic activity of neurons, and therefore may indicate areas of brain damage
- Functional magnetic resonance imaging (fMRI) provides a picture of how people react to stimuli virtually in real time, making it possible to present stimuli to an individual while the examiner monitors the individual's response.
- Summary
- A psychological assessment is a procedure in which a clinician provides a formal evaluation of an individual's cognitive, personality, and psychosocial functioning. Clinicians conduct assessments under a variety of conditions. In many cases, clinicians use the assessment process to provide a diagnosis, or at least a tentative diagnosis, of an individual's psychological disorder.
- To be useful, clinicians must hold assessments to standards that ensure that they provide the most reproducible and accurate results. The reliability of a test indicates the consistency of the scores it produces. The test's validity reflects the extent to which a test measures what it is designed to measure.
- Clinicians should use the best assessment methods possible. Evidence-based assessment includes (1) relying on research findings and scientifically viable theories; (2) using psychometrically strong measures; and (3) empirically evaluating the assessment process.
- The clinical interview is a series of questions that clinicians administer in face-to-face interaction with the client. The answers the client provides to these questions provide important background information on clients, allow them to describe their symptoms, and enable clinicians to make observations of their clients that can guide decisions about the next steps, which may include further testing. The format can be structured or unstructured.
- A clinician uses a mental status examination to assess a client's current state of mind. The clinician assesses a number of features of the client including appearance, attitudes, behavior, mood and affect, speech, thought processes, content of thought, perception, cognition, insight, and judgment. The outcome of the mental status examination is a comprehensive description of how the client looks, thinks, feels, and behaves.
- Intelligence tests such as the Stanford-Binet Intelligence Test, but particularly the Wechsler scales, provide valuable information about an individual's cognitive functioning.
- Clinicians use tests of personality to understand a person's thoughts, behaviors, and emotions. There are two main forms of personality tests: self-report and projective. Tests include the Minnesota Multiphasic Personality Inventory (MMPI), the Personality Assessment Inventory (PAI), the SCL-90-R, the NEO Personality Inventory, and other specific self-report inventories designed to investigate specific disorders or research questions for which a general test may not be relevant.
- Unlike psychological tests, behavioral assessments record actions rather than responses to rating scales or questions. The target behavior is what the client and clinician wish to change. Behavioral assessments include descriptions of the events that precede or follow the behaviors. In vivo observation takes place when clinicians record behavior in its natural context, such as the classroom or the home. Analog observations take place in a setting or context such as a clinician's office or a laboratory specifically designed for observing the target behavior. In a behavioral self-report the client records the target behavior, including the antecedents and consequences of the behavior. Self-monitoring is a form of behavioral self-report in which the client keeps a record of the frequency of specified behaviors.
- When psychologists conduct a multicultural assessment, they must take into account the person's cultural, ethnic, and racial background.
- Neuropsychological assessment is the process of gathering information about a client's brain functioning on the basis of performance on psychological tests. Clinicians use neuropsychological assessment measures to attempt to determine the functional correlates of brain damage by comparing a client's performance on a particular test with normative data from individuals who are known to have certain types of injuries or disorders. There are a variety of tests to assess verbal recall and auditory attention. Physiological measures include brain imaging techniques such as EEG, CT scan, MRI, fMRI, PET, and other techniques for assessing abnormalities in the body, particularly the brain.







