Kyasanur Forest Disease (KFD): Clinical Presentations, Diagnosis, Treatment And Prevention

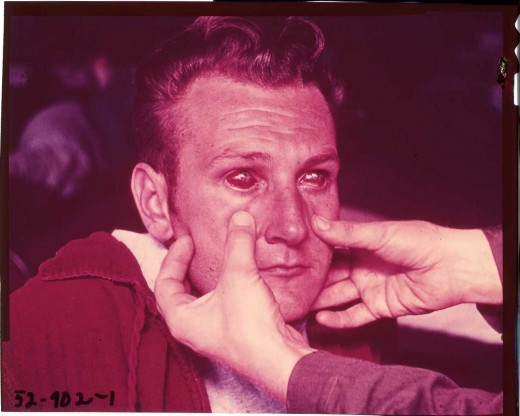
The Physical Presentation Of Kyasanur Forest Disease
Kyasanur Forest Disease
Kyasanur forest disease (KFD) is an acute febrile illness caused by a group B arbovirus, clinically characterized by sudden onset of fever with rigor, severe body pains, headache, meningism, delirium, mental confusion and dehydration. The original description was from Shimoga district of Karmataka state in South India in 1956.
The disease was prevalent among people living in the villages around the forest area. The infection developed in persons who has gone into the forest (usually to fetch wood) and who had come into contact with dead monkeys. The ticks Hemaphysalis Spinigera and Ixodes act as vectors to transmit the disease from animals to man. Monkeys (black faced langur and macaques), Shrews and rats are known to harbour the virus. Man gets infected by the bite of the nymph of H. spinigera. Infected ticks carry the virus for long periods. Personnel working in laboratories handling the virus or investigators working in the affected areas are susceptible to infection. In addition to vector transmission, infection can also be spread by inhalation of infected material.
Hemorrhagic Presentations In Kyasanur Forest Disease

Infectious Diseases

Clinical Features Of Kyasanur Forest Infection
After the incubation period lasting for 2 to 7 days, sudden fever sets in with chills and rigor. Fever is associated with headache and severe myalgia in the nape of the neck, back and calf. These may be mistaken for dengue fever. Abdominal pain, diarrhea and vomiting may occur between the third and the seventh day. Uncommonly, bleeding tendencies such as epistaxis, bleeding gums and melena may develop around the third day. Lymphadenopathy of the neck and axilla, and conjunctival injection may also be seen. Bradycardia and hypotension may develop. Hepatosplenomegaly may occur in some cases. Alteration in mental state, neck rigidity, giddiness, tremors, listlessness and dyspnea have all been reported.
In uncomplicated cases, the fever lasts for about 10 to 12 days and temperature comes down. A second febrile phase may follow 2 to 12 days after the temperature has touched normal and this may continue so for 9 to 21 days. The mortality rate is around 5%. Death is usually caused by pulmonary edema.
Laboratory diagnosis: Leucocyte count is low (about 3000/cmm). The virus can be isolated from blood during the course of the fever. Paired sera show rise in antibody titers. During the second febrile phase, CSF may show features of aseptic meningitis.
Treatment: In the absence of specific treatment only supportive therapy is to be given.
Prevention: Anti-tick measures have to be instituted during jungle clearing operations. Persons at risk should use protective clothing and insects repellants. Though a vaccine was developed against KFD, it was not found to be very effective.
© 2014 Funom Theophilus Makama


