Obesity, Diabetes and Bariatric Surgery

Obesity is officially one of the most pressing public health problems in the world. It has been a leading health problem for many countries of the west for many years now and World Health Organisation (WHO) statistics show that this problem is growing at an alarming rate in urban areas of almost all developing countries.

Obesity and Diabetes
Obesity and Type 2 diabetes, also known as adult-onset diabetes, go hand in hand. This is no mean challenge. Diabetes is arguably the most formidable chronic illness an individual can have. Diabetes can and does affect practically all body systems but most notably the cardiovascular system, the kidneys and eyes. Diabetes does increase the risk of some malignancies associated with obesity. We already know that obesity on its own may be responsible for a third of all breast cancer cases. Now, a recent study has revealed that breast cancer diagnosis in the presence of pre-existing diabetes does increase the chances of dying from the disease by as much as 50%. It is a toxic mix.
Apart from a lifetime of ill-health, there is now evidence that, when it comes to overall mortality, obesity, especially extreme obesity, is at par with smoking. A report in the Lancet Medical Journal in March 2009 showed results of a study that indicated that median survival is reduced by 8 to 10 years when the BMI is in the 40-45 range (BMI calculator here:)
Obesity and ill-health
One of the commonest challenges every physician has to deal with is to confront the issue of obesity in a constructive way so as to keep the patient on board when doing a consultation. This is actually harder than you might think. People with a problem of obesity struggle not only with the health consequences of the condition but also with discrimination socially and in the workplace and the last thing they need is a perceived similar treatment at the hands of a healthcare worker. It is therefore unsurprising that many assume a defensive mode at the slightest mention of the ‘f’ word. For a gynaecologist and obstetrician like me, the patient may present with problem of pelvic pain, menstrual problems, sub-fertility, sexual health issues, pregnancy complicated by diabetes, urinary incontinence, pre-cancerous conditions or a combination of many of these. You somehow have to find a way of pointing out the elephant in the room (pun completely unintended), as it is quite often at the core of the presenting problem.
Statistics, statistics and damn statistics
Let’s take a brief look at the facts: In 2006, almost a quarter of the adult
population (over 16 years of age) in the UK were classified as obese with 1% of
men and 3% of women being morbidly obese (BMI over 40). By 2012, it is
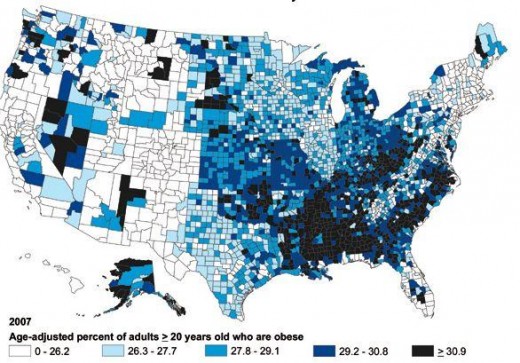
estimated that over 33% will be obese. In the United States, the prevalence of
obesity varies by state (see map below) with states like Colorado having less than
20% and other states like Alabama, West Virginia, Mississippi, Louisiana and
several others having levels over 30%. There are racial differences too with
Blacks having 51% higher prevalence of obesity, and Hispanics 21% higher obesity
prevalence compared to whites. The United States stands out, however, on the
significantly higher levels of morbid or extreme obesity. Levels of morbid
obesity increased
50% between the years 2000 and 2005. There is no evidence that this trend
is slowing down. In India, a study by the Indian Diabetes Foundation in 2010 revealed that a third of children in private schools in the capital New Delhi were obese, on track to become obese and diabetic adults. The demographic difference with developed countries where obesity and poverty go hand in hand, in India and other developing countries, this is a problem of the well-off middle classes.
Obesity in the USA
Towards diabetes
According to WHO, there are 285 million people with type 2 diabetes worldwide, and this figure will rise to 438 million by 2030 with an additional half a billion people at risk. Diabetes is a major chronic health problem and obesity fuels this. The risk for type 2 diabetes is dramatically increased in individuals who are severely obese. For men, the risk of type 2 diabetes is increased 42 times compared to individuals of normal weight while for women the increase is a mind-boggling 93 times. In percentage terms, that is a 9300% increase!
The International Diabetes Federation (IDF) puts the lifetime cost of diabetes in the United States at $172,000 for a person diagnosed at age 50 years and $305,000 at age 30 years. That is a serious amount of money by any measure and a completely unattainable public health commitment in developing countries. Results of conventional medical treatment for Type 2 in the presence of significant obesity (BMI over 30) are disappointing even in places where this is at a cutting age. One recent Swedish study showed success (i.e. diabetes remission) in only 13% of cases.
Bariatric surgery in Type 2 Diabetes
Bariatric surgery is performed with the specific aim of reducing food intake as a way of reducing weight. There are various procedures performed to achieve this including banding gastroplasty (reduce size of stomach pouch using a restrictive band), stapling gastroplasty (also reduce size of stomach pouch by stapling), partial gastrectomy (resecting and removing part of the stomach pouch) and a few other bypass procedures. All achieve the same thing by forcing the individual to eat less as there is restricted space in the stomach. This hub is not meant to go into details of what and how this is done. That information can be accessed elsewhere.
There has been an explosion of bariatric surgery all over the world to deal with obesity. It is, of course, unlikely that surgery by itself will have a significant impact on the overall prevalence of extreme obesity. However, at an individual level, the impact can be transformational. Recent studies show that successful bariatric surgery leads to remission of the diabetes in 73% of cases. Yes, bariatric surgery isn’t always successful, can have complications and is expensive (cost estimated at $20,000 -30,000) but compared to the health toll of a lifetime of obesity, the upside is a lot bigger.
Whilst each individual needs to look at adjusting their lifestyle to prevent morbid obesity and/or diabetes; where one or both conditions are already established, bariatric surgery is a legitimate and often the superior option to aim for.



, Know the Risk factors")


