Understanding Headache - What should be done when you get a headache?


Headache is one of the commonest causes for visits to the out patient departments (OPD) of the hospitals and the primary care physicians accounting for 22 consultations per 1000 population per year in the UK. Tension headache, one of the commonest forms of headache is said to affect 86% of women and 63% of men every year. It is often incapacitating but only rarely is it caused by a potentially serious illness. As it is so common, it is often ignored and reassured even when it is a symptom of a sinister disease. Therefore, it is important to know about headache and when to go to a doctor seeking treatment.

For the convenience of understanding headaches can be classified into several groups.
1. Acute single headache
2. Recurrent headaches
3. Triggered headaches
4. Dull aches increasing in severity
5. Dull aches persisting for months
Acute single headaches are the commonest of all and most of the time, are benign. The commonest causes of a single episode of headache include benign (harmless) causes like tension headache, headache associated with fever, sinusitis and first attack of migraine and sinister (harmful) causes like injury to the head, intra-cranial haemorrhage, stroke and meningitis. The commonest cause of recurrent headaches is migraine. In addition, cluster headaches, episodic tension headaches and certain neuralgic syndromes (e.g. – trigeminal neuralgia and post herpetic neuralgia) can give rise to recurrent headaches. Triggered headaches are almost always due to migraine with the triggering factors being exertion, stress, relief from stress, certain items of food such as cheese and chocolate, travelling and sexual intercourse. Dull headaches increasing in severity are also benign most of the time and may be due to any cause of pain in the head and neck region (e.g. – neck pain, tooth aches) but can be due to sinister causes such as temporal arteritis which can lead to irreversible blindness and brain tumours. Dull aches not changing in severity are the chronic tension headache and the headaches associated with depression. How to recognize the sinister headaches is dealt with in a separate article by the author and here the readers are given glimpse of some common types of headaches seen in day to day life. Migraine being a disease that is common but difficult to treat is dealt-with in a separate article.
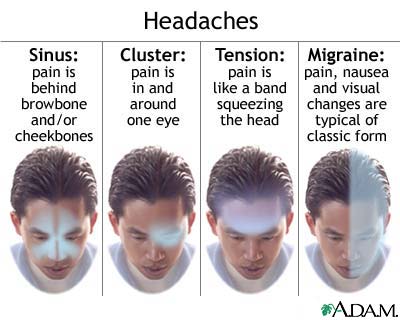
Tension-type headache
Most are seen to suffer from attacks of non-throbbing headache occurring simultaneously on either side of the head. Even though this is not as incapacitating as migraine, about 5% of those affected are seen to have a continuous, chronic headache. Most never seek medical advice and depend on over-the-counter analgesics. Investigations are almost always unnecessary. Many of the patients who present for medical care are taking analgesics (e.g. ergotamine, codeine, caffeine) on a daily basis, and it is now proven that their headaches often settle when theses drugs are withdrawn – suggesting that the analgesics are the cause for the headache. In some patients, headache may be due to the contraceptive pill or hormone replacement therapy (HRT). Others (particularly those with chronic headache) are overtly depressed, and are often cured completely with tri-cyclic antidepressants (e.g. – Amitriptylin). However, current practice is to minimize the use of medication as much as possible in chronic tension headache though analgesics like paracetamol (acetaminophen) and non-steroidal anti-inflammatory drugs (e.g. – diclofenac sodium, aspirin) may be used. Reassurance of the patient is an important part of the management and advice to reduce the level of stress and avoidance of unhealthy postures may be important.
Sinusitis
Headache and facial pain are commonly seen in acute viral infections such as the infection with influenza. A single episode of severe headache following a common cold may be caused by secondary bacterial infection in the frontal or maxillary sinuses. Patients may experience pain and tenderness over the sinuses and a post-nasal drip and bad odor of breath may suggest the presence of the illness. This can be confirmed by skull radiography and usually resolves with oral antibiotic treatment.
Cluster headache
Cluster headache syndromes are less common than migraine. Being commoner among men unlike most other types of headaches, episodes of unbearably severe, steady pain, usually in the eye, cheek or temple on one side only, may be experienced lasting between 30 minutes and 3 hours, often several times daily. Patients are usually seen to wakeup from sleep, due to the severity of pain. The episodes are often accompanied by autonomic disturbances such as drooping of eyelids, excessive tearing from one eye, redness of one eye and watering or blockage of the nostril on that side. In most of the patients, the pain occurs daily for 6–12 weeks, after which there is a remission that may last from 3 months to 2 years before recurrence of a similar episode. Investigations are often unnecessary if the history is suggestive, although the syndrome is occasionally mimicked by structural disturbances in the pituitary gland or cavernous sinus.Therefore atypical patients should undergo CT or MRI of the brain.
Management of cluster headaches is difficult. Inhalation of 100% oxygen and subcutaneous sumatriptan, or sumatriptan or zolmitriptan administered by nasal spray may be effective. However, prophylactic treatment is the mainstay of management; verapamil is the drug of choice of choice, though patients also respond to lithium carbonate, ethysergide and gabapentin. Corticosteroids (e.g. –prednisolone) are effective, but perhaps to be recommended only in patients in whom previous experience suggests that the cluster is likely to end within 2 or 3 weeks. Surgical destruction of the trigeminal nerve can be implemented in those who fail to respond to other modalities of trement.
Trigeminal neuralgia
Trigeminal neuralgia is commonly seen in old age. The pain is thought to be caused by compression of the trigeminal nerve by an abnormally placed artery at the point the nerve leaves the brainstem. The compression may also be due to a plaque of multiple sclerosis or an aneurysm in the arteries. The pain is described as severe, knife-like, lasting only 1 or 2 seconds, and being confined to the distribution of the trigeminal nerve on one side, especially over the cheeks (maxilla) and the mandible. Attacks are often triggered by chewing, eating, speaking or touching the face, or even by the wind. Carbamazepine and gabapentin are often effective in most of the patients though ablation of the nerve or corrective neurosurgical procedures to wrap the artery or an aneurysm if present may be necessary.
Atypical facial pain
Atypical facial pain is less well localized in the face unlike trigeminal neuralgia which is well localized. The pain often lasts longer and may be continuous. All other causes of headache and facial pain should be excluded before arrival at the diagnosis and it is important for the patient to be screened by a dental surgeon, ENT surgeon and ophthalmologist. Many patients with atypical facial pain are depressed, and therefore tri-cyclic antidepressants are effective in the treatment.
Other causes of headache
Paget’s disease of the skull is an uncommon cause of headache in older patients. Although chronic hypertension can give rise to headache, especially when diastolic blood pressure exceeds 140 mm Hg, it is a rare cause of headache. In contrast, paroxysmal hypertension, which may be caused by phaeochromocytoma, and severe hypertension may present with a severe headache associated with vertigo.







