Understanding Heart Failure - A Complete Account

Heart failure is a complex syndrome that develops when the heart fails to maintain an adequate cardiac output (out put of blood per minute from the heart) to provide all organs with blood supply appropriate to demand, occurring due to any structural or functional cardiac disorder. It is a common condition seen in 1% in the age group of 50-59 years and becoming commoner to 5-10% in 80-89 the age group of years. Two to four percent of the individuals less than 65 years and 10% of the individuals above 65 years are seen to develop heart failure annually. It is known to cause death in 50% of the diagnosed patients within 5 years and is responsible for 5% of the total number of hospital admissions to medical wards.
Causes for heart failure are multiple and are discussed in detail in a separate article by the author along with pathophysiology and pathogenesis of heart failure. Basically, the causes can be classified in to
1. Impaired contractile function of the heart (impaired pumping action)
2. Obstruction (blockade) at the out flow tract from the heart
3. Obstruction (blockade) at the in flow tract from the heart
4. Unusually high volume of blood in circulation
5. Arrythmias (rhythm abnormalities of the heart)
6. Diastolic dysfunction (impaired filling of the heart due to the inadequate size)
Heart failure is classified into various syndromes based on anatomy, temporal nature and physiology. Anatomically heart failure is divided into left heart failure (LVF), right heart failure (RVF) and bi-ventricular failure. Symptoms of left heart failure include fatigue, shortness of breath on exertion (exersional dyspnoea), shortness of breath when lying down (orthopnoea) and recurrent disturbances to sleep when lying down at night (paroxysmal nocturnal dyspnoea). On examination the cardiac apex may be displaced and elevated with abnormal 3rd and 4th heart sounds (gallop rhythm) and fine crackles over the lung bases. Right heart failure usually presents with fatigue, nausea and vomiting with swelling of the dependent parts of the body (e.g.- ankles). On examination, jugular venous pressure may be elevated with tender enlargement of the liver. Bi-ventricular failure is the presence of left and right heart failure at the same time.
Based on the temporal nature heart failure is classified into acute n chronic heart failure. Acute heart failure is characterized by acute on set shortness of breath with features of collection of fluid in lungs. Clinical features include acute breathlessness, wheezing, anxiety and profuse perspiring with a cough producing pink (blood-tinged), frothy, copious sputum. Heart rate and respiratory rate may be abnormally high. Examination may reveal crackles and rhonchi through-out the chest with abnormal heart sounds and murmurs. Chronic heart failure is a remitting and a relapsing course of the above presentation with intermittent periods of stability (compensated heart failure).
Going by the guidelines of European Society of Cardiology, diagnosis of heart failure is based on two essential features,
- Symptoms & signs of HF (breathlessness, fatigue, ankle swelling)
- Objective evidence of cardiac dysfunction (at rest) – and
- Response to Tx directed towards HF (when doubtful)
The severity of heart failure is determined clinically by the New-York Heart Association Guidelines for Severity.
– Grade 0 – normal
– Grade I – dyspnoeic on heavy exertion (weight lifting, cutting wood)
– Grade II – dyspnoeic on moderate exertion (climbing steps)
– Grade III – dyspnoeic on mild exertion (walking, sweaping)
– Grade IV – dyspnoeic at rest
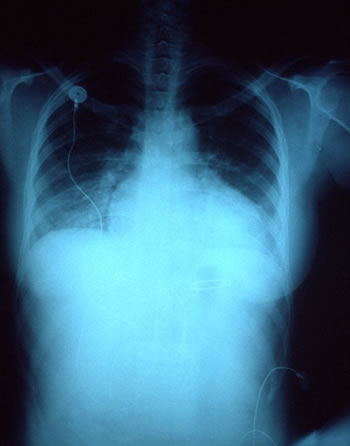
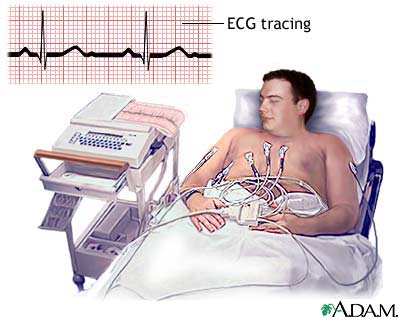
Certain investigations may be necessary in order to diagnose heart failure and may include a chest X-ray, blood investigations such as blood cell counts, serum electrolytes, cardiac enzyme levels and thyroid function test, ECG and echocardiography. Additional diagnostic investigations such as stress echocardiography – exercise / pharmacological, nuclear cardiology (SPECT), cardiac MRI, PET, cardiac catheterization and cardiac biopsy may be necessary if the diagnosis or the causative factor is not straight forward. The outcome (prognosis) is assessed by cardiopulmonary exercise testing, ambulatory (24-28 hour) ECG monitoring and resting & stress radionuclide angiography (MUGA).
Complications of heart failure include renal (kidney) failure aggravated by the drugs in the long run, electrolyte imbalances, impaired liver functions and thrombo-embolism (deep vein thrombosis and pulmonary embolism due to impaired activity). Rhythm abnormalities (arrhythmias) can occur and may lead to sudden death if not treated properly.
Management of heart failure is complex and is discussed in a separate article by the author. However, the management of chronic heart failure is a multi disciplinary approach like in any other chronic condition with patient education, life style advice and a good follow-up program. Drugs and other non-pharmacological techniques may be necessary for further management of the patients. Special interest should be given for the management of acute heart failure in such patients as it can be life-threatening. Being a condition which is not curable but only manageable, it is important to diagnose the disease early and control the progression of the disease with proper life-style and medical management to increase the quality of life of the patients.







 - When The Heart Skips a Beat")