Common Sense Look at Marijuana as a Gateway Drug


Preface
The following essay takes a critical look at marijuana as a gateway drug, its ambiguous role in society and what this means in day to day practice. If we actually care about problems in the world related to substance use, we have to phrase the problem correctly and take many other factors into account. I begin by posing a few questions to help us understand what we actually mean by “gateway” followed by a discussion about how one might look for evidence of this in the data that we have.
Corpus
Is the term gateway meant to be a cautionary label? Where do the concepts of dependence and gateway overlap? The term gateway implies a transition from one category of drug use to another. To make the gateway argument work, we have to think about it in terms of the desire to achieve more effective qualities of mind alteration. i.e. dependence. You could also make the case that marijuana is the first stepping stone among many in the pursuit of higher highs. Using this low-resolution description, we still have to contend with the assumption that by removing the “first stepping stone”, we could somehow reduce future use of other illicit substances. I see no evidence of that and rates of marijuana use by 12th graders today are still only half what they were in 1978 (Hart & Ksir, 2014 p.7) yet we still currently have fluctuating issues with hard drugs in the U.S. We would also expect to see marijuana trend lines marionetting the use trends of other illicit drugs.
Percentage of College Students One to Four years beyond High School Reporting Use of Seven types of Drugs
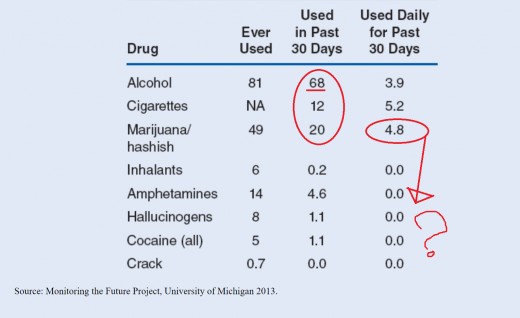
The graph above shows us several important things. First, the most used substance over the past 30 days is overwhelmingly alcohol by a factor three times more than that of marijuana. Interestingly, when we move the scope to everyday use, we find tobacco use exceeding that of both marijuana and alcohol which are nearly on par with one another. While daily use of marijuana is higher than alcohol, we hardly see any effect on the use of other substances and even less on the daily use scale. If marijuana allegedly pushes people in the direction of other drugs, it’s not reflected here. Also, data derived from college-age students is significant because if we accept that marijuana use begins sometime before the age of 18, we should see an interesting transition to other substances on graphs designed to monitor the use of specific drugs in those populations. I don’t think I’m using the wrong metric here. I see alcohol, tobacco, and marijuana remaining steadfastly popular with other drug use happening within a very small minority of people. And, if there is a significant correlation between the three most prevalent substances, the data we have can’t say which one of the three or combination thereof could explain the gateway phenomenon.
(SAHMSA, 2013) says, “More than half of new illicit drug users begin with marijuana”. So, if someone tries crack cocaine at the age of 35 and reports having used marijuana at age 15, are we also to assume that trying marijuana is ultimately what set him on a twenty-year path that could not have resulted in anything other than the use of crack? I could see this being the case in the small proportion of people with bipolar I disorder. But what about trauma? Lack of education? Criminal influences? Incarceration? Mental disorders? Why are we forgoing the kinds of questions needed to explain why humans do the things they do? Maybe it’s as simple as: people who are likely to take the risk of experimenting with marijuana are also of the sort to take risks in general. That seems like a psychologically (and biologically) sound explanation to me – adolescence!
Let’s think of this problem another way. Remember that the use of alcohol has an inhibitory effect across cognition, emotion and motor output (Hart & Ksir, 2014 p. 203). Suppose I wanted to make the argument that because of these effects, alcohol causes people to become more violent or dangerous. It would be positively fatal to my master’s thesis if I actually tried to imply causation to something in this way despite the fact that we see alcohol as a common factor in many (maybe most) violent crimes (NIH, 2000). I have to think about the cause and effect of behavioral traits such as aggression in terms of pre-existing proneness and a combination of other things like age, sex, background, etc. The same principle would have to apply to the issue of marijuana as a gateway drug in its most general sense. What I see is a buzzword that’s carried a lot of political gravitas over the years but has yet to explain much of anything about marijuana’s actual role in society. The jury is arguably still out for deliberation in that regard.
My most honest answer to whether or not I believe marijuana is a gateway drug is: “I don’t know”. Why do antidepressants make some people more depressed and suicidal? But, that fact still doesn’t compel me to strip them from the market altogether or assume that this side effect happens in more than just a small minority of people who take them.
What are we really talking about here? The real dangers of marijuana can be delineated readily. There's no conspiracy to cast smog over otherwise legitimate health concerns.
- Marijuana raises heart rate (Hart & Ksir, 2014 p. 364) which is obviously hazardous to hundreds of thousands of people who suffer from heart attacks each year (CDC, 2017).
- Marijuana impairs coordination (Hart & Ksir, 2014 p. 359) in similar ways to alcohol and we don’t want people operating heavy machinery under its influence.
- In a more recent assignment, I described how the use of marijuana can actually trigger the onset of psychosis in individuals who are genetically prone to developing schizophrenia (Kaminer, 2016).
- …Causes anxiety (Hart & Ksir, 2014)
- …Diminishes sperm count (2014)
- …Is implicated in diseases of the respiratory system similar to that of long-term tobacco use… (2014)
These are just a few of the concerns I would have when evaluating clients in the future. At the very bottom, it would be inadvisable to recommend that anyone inhale combustible material. Some people are going to choose to do these things anyway. Our job as future practitioners in this field is to facilitate change in a myriad of ways including general risk reduction. If someone quits drinking alcohol and begins smoking marijuana instead, I would not tell them it would be better to go back to drinking alcohol but I wouldn’t encourage long-term use of marijuana either. If I took the gateway concept seriously I would have to be concerned that this particular alcoholic will now be putting themselves at risk for other drug use from that point forward. It’s not clear to me that he wasn’t at risk for other drug use to begin with.
Lastly, why is the transition from legally prescribed opiates to heroin use and subsequent fentanyl use of no concern? Isn’t it true that some people who originally take opiate medication for pain find themselves helplessly “crossing the gate”, as it were, into a world of more potent drugs? Even then, we cannot place the blame squarely at the feet of the pharmaceutical industry or the pills themselves. We have to talk about these things using well-established systems analysis. In psychology, we break the problem down into smaller pieces and examine the relationships between them at the level of genes, mental health, and the environment.
References
CDC (2017) Heart Disease Facts. Retrieved from https://www.cdc.gov/heartdisease/facts.htm
Hart, C. & Ksir, C. (12/2014). Drugs, Society, and Human Behavior, 16th Edition. [Purdue University Global Bookshelf]. Retrieved from https://purdueuniversityglobal.vitalsource.com/#/books/undefined/
Johnston, L. D., O’Malley, P. M., Bachman, J. G., Schulenberg, J. E., & Miech, R. A. (2014). Monitoring the Future National Survey Results on Drug Use, 1975-2014. Monitoring the Future: National Survey Results on Drug Use, 2, i. Retrieved from http://search.ebscohost.com.libauth.purdueglobal.edu/login.aspx?direct=true&db=edb&AN=110121673&site=eds-live
Kaminer, Y. (2016). Youth Substance Abuse and Co-occurring Disorders (Vol. First edition). Washington, DC: American Psychiatric Publishing. Retrieved from http://search.ebscohost.com.libauth.purdueglobal.edu/login.aspx?direct=true&db=nlebk&AN=1610205&site=eds-live
NIH (2000) National Institute on Alcohol Abuse and Alcoholism. Retrieved from https://pubs.niaaa.nih.gov/publications/aa38.htm
SAMHSA (2013) Results from the 2013 National Survey on Drug Use and Health: Summary of National Findings. Retrieved from https://www.samhsa.gov/data/sites/default/files/NSDUHresultsPDFWHTML2013/Web/NSDUHresults2013.htm#3.1.2
Related

How Does a Drug Addict Think, Feel, and Behave While Actively Addicted?
 and Sources of Drug Information")
Pharmacological Effects, Prodrugs (Definition, Examples) and Sources of Drug Information

Absorption of drugs: how drugs are absorbed in the body? ePharmacology

Is There Any Issue of Mistrust or Culture of Silence in Ghana’s 2020 Elections Petition?

Loving a Drug Addict - My Story of Living With and Loving a Meth Addict.


