How close are we to preventing psychosis?


What is psychosis?
In psychiatry, there are two main types of disorders; psychoses and neuroses. Neurosis, considered milder than psychosis, describes disorders where the insight of a patient is retained. In psychosis however, a patient normally loses insight (is not aware of the disturbance in their thinking patterns). Patients diagnosed with psychosis would be expected to have at least one of the three following symptoms:
- Delusion; where the patient has beliefs which are false and usually contrary to what they have been taught during upbringing and from their background. This belief is not affected by any form of reasoned argument.
- Illusion; where the patient makes misinterpreted perceptions.
- Hallucination; where the patient makes false perceptions of their surroundings without an external stimulus.
Psychotic disorders affect a person’s ability to think clearly, possibly affecting their ability to make judgements, produce an emotional response, communicate, and in more severe cases, their understanding of reality. They distort a person’s senses causing confusion as to what is real. Psychotic disorders affect a significant number of people all over the world, both men and women equally, often striking in their late teens and early 20’s.
It is estimated that about 3 people in every one hundred experience a psychotic episode in their lives; this ratio makes psychosis more common than diabetes. However, most people do make a full recovery, although early assessment, education, and treatment are necessary and greatly improve the outcomes for the individuals and their families.
There are a number of types of psychotic disorders, they include:
- Shared psychotic disorders
- Schizophrenia
- Schizoaffective disorder
- Schizofreniform disorder
- Brief psychotic disorder
- Delusional disorder
The symptoms of psychotic disorders vary from person to person and often change over a period of time; as mentioned earlier, the main ones are hallucinations and delusions; however others include:
- Incoherent speech
- Strange or even dangerous behaviour
- Confusion
- Slow or unusual movements
- Problems in maintaining relationships
- A loss of interest in personal hygiene
- A loss of interest in daily activities
- An inability to express emotions
- Mood swings
Causes of psychosis
Psychosis is a serious mental illness which can be the result of a physical health problem or disease, such as UTI’s and chest infections in the elderly, and brain diseases which include Parkinson’s, dementia, and epilepsy. The exact causes of psychotic disorders are not completely understood; however some of the disorders are known to run in families, some have been associated with certain environmental factors such as stress and drug abuse; others seem to occur due to a chemical imbalance in the brain which affects the brain’s response to certain stimuli.
It is vital that we clearly understand what can potentially cause psychosis if we hope to, in the future, prevent it before the occurrence of the first episode. Factors which contribute to the development of psychosis can be genetic or environmental.
Environmental factors
Possible environmental factors of psychosis being investigated include the deficiency of vitamin D which plays a role in brain development. It has been noted that schizophrenics with psychotic symptoms have low levels of vitamin D; this can be tackled by administering vitamin D S supplements. The functionality of mitochondria is also being investigated, as it is the organelle which provides energy to cells, including those in the brain. Without the right amount of energy, the cells wouldn’t function as they normally would; this could be potentially avoided by the intake of several vitamins and minerals. People with schizophrenia as well as those with bipolar disorder have been found to have malfunctioning mitochondria.
Numerous studies have shown a correlation between the occurrence of psychotic disorders and other factors. For example, complications at birth as well as growing up in a large city seem to play a role in the development of schizophrenia, while trauma during childhood and stressful events play a role in the development of both schizophrenia and bipolar disorder. Unfortunately there isn’t much we can do to prevent such things from happening in an individual’s life. There are many other potentially contributing factors which we are still unaware of.
Genetic factors
There have been hundreds of studies conducted to investigate whether and to what extent psychosis can be passed on genetically. So far, researchers have concluded that the disorder is not entirely ‘genetically distinct;’ this means that there aren’t any specific genes which cause it, however there are those which increase the chances of it developing if the disorder was to be triggered by another factor. Scientists believe that it is the combination of genes and life experiences which determine which illness is most likely to develop in an individual; this means that theoretically, psychosis can be completely avoided if the individual has the correct lifestyle.
Biochemical levels in the brain
One factor which seems to be most directly linked to the occurrence of psychosis is the level of dopamine in the brain. Dopamine is one of many neurotransmitters -chemicals that pass information from one neuron (brain cell) to another. It plays an important role in memory, problem solving, attention, and the control of movement. Dopamine is normally released in the brain as a result of rewarding experiences; it is also found in most illegal drugs.
Research has shown a clear correlation between high levels of dopamine and hallucinations, delusions, and disordered thoughts. The level of dopamine is normally at its highest just before first episode psychosis. Its levels can normally be controlled by taking dopaminergic drugs to increase its quantities in the brain or by taking dopamine antagonists to reduce its quantities.
The level of dopamine is referred to as ‘the final common pathway’ to psychosis. This means that it is what links events in an individual’s life to the actual development of psychosis. The exact mechanism by which the rise in dopamine levels is caused, as well as how the rise causes psychosis, is still unknown. It is possible that by regulating the levels of dopamine, one can avoid the occurrence of psychosis without having to alter their lifestyle.
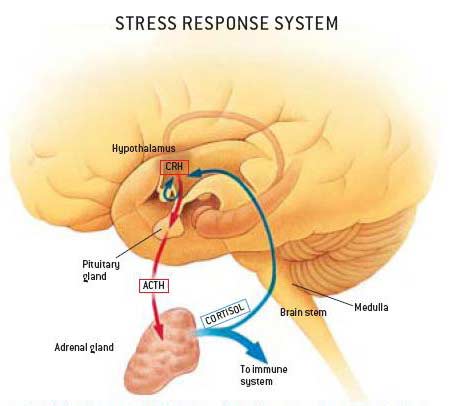
Stress is one of the main factors which are linked to the development of psychosis. Psychotics tend to find dealing with stress very challenging. When an individual experiences stress, cortisol, a hormone, is produced by the adrenal glands. The production of the stress hormone is controlled by the hypothalamic pituitary adrenal (HPA) axis, a system which is made up of the hypothalamus, the pituitary glands, and the adrenal glands; these are shown in the diagram on the right. Abnormally high levels of cortisol are normally detected in people experiencing first episode psychosis, suggesting the existence of a link between the two. It has been noted that the higher the levels of the hormone, the more extreme the symptoms as the presence of high levels of cortisol is known to increase the production of dopamine which causes the mental illness. Therefore, reducing stress levels should theoretically reduce the risk of developing psychosis as well other health complications.
Continuous high levels of cortisol have a negative effect on the hippocampus, which is the part of the brain responsible mainly for short and long term memory as well as spatial awareness. This theory is supported as it is evident from brain imaging that the volume of the hippocampus in a schizophrenic individual is smaller than that in a non-schizophrenic individual. It has been noted that blood relatives of people who experience psychosis are also more sensitive to stress than the average individual, as they too have an overactive HPA axis which causes an overabundance of the neurotransmitter dopamine. Research has been conducted to investigate this however there is not enough evidence to confirm that the hyperactivity of the HPA axis is genetic.
Research and Studies
In the last few years, several studies have been undertaken to investigate the link between childhood adversity and the occurrence of psychosis in an individual. A team of scientists from the Institute of Psychiatry published a study in February 2010 in which they collected and analysed information from a large number of people who had experienced first episode psychosis; over 12% of the individuals reported to have suffered from physical abuse by their mothers before the age of 12. A sample of people who did not have psychosis was also surveyed of which only 4% reported the same form of abuse.
A research team analysed information from 7353 people in the Adult Psychiatric Morbidity Survey in England in 2007 to find that sexual abuse before the age of 16 is strongly correlated with the development of psychosis in later life.
Another team examined results obtained from 36 different studies recently carried out. These studies involved about 80,000 people; after analysis, they found that individuals who had experienced abuse and trauma as children are about three times more likely to develop psychotic symptoms in their life than those who had not experienced it.
There is a strong correlation between the two however it is not always the case; as mentioned earlier, there are many factors which can cause these symptoms. The cases of abuse or trauma merely affect the brain’s methods of coping with the stresses of everyday life which in turn may give rise to psychotic symptoms.
Diagnosis
Neurologic examination is an essential process in diagnosing patients with psychiatric disorders. They consist of different complex and challenging components. Conducting such tests requires many skills which can only be mastered by the repeated use of the necessary techniques on people with, as well as without neurologic diseases. Many cases go undiagnosed; it is essential that we change this in order to prevent potential future episodes.
Most clinicians begin the process with an assessment of the patients’ mental status followed by their cranial nerves, their motor system, their sensory system, their coordination, and finally, their gait. A patient’s mental status is examined by observing their communication abilities (i.e. speech), memory, orientation, and level of consciousness. Their cranial nerves are assessed by checking the fundi, visual fields, pupil size, and extra ocular and facial movements. For the motor system, the clinician would look for muscle atrophy. To examine the sensory system, the patient is asked whether they can feel a light cool touch on their skin. For the assessment of the patient’s coordination, the patient’s ability to perform rapid movements is tested. Finally, for a patient’s gait, observations are made while the patient is walking normally, along a straight line, and on heels and toes.
Detecting abnormalities is difficult as we cannot do biopsies of different sections of the brain as we normally do with other organs.
Urine sampling and blood tests provide no room for disagreement amongst physicians when diagnosing patients with disorders such as diabetes. However, before these tests were used, there was a lot of uncertainty as to which diagnosis is most suitable. It is this stage which we are at now with the diagnosis of psychiatric disorders.
There are a number of other tests which we may be able to use to help with the diagnosis of such disorders. Over the last few decades, there have been huge advances in neuroimaging leading to an expanding number of options which include:
- CT (computed tomography)
- CT angiography (CTA)
- Perfusion CT (pCT)
- Magnetic Resonance Imaging (MRI)
- Functional MRI (fMRI)
- MR spectroscopy (MRS)
- MR neurography
- Diffusion and diffusion track imaging (DTI)
- Perfusion MRI (pMRI)
Using these advances makes the diagnosing of mental illnesses significantly more straightforward.
Having an MRI can prove to be very intimidating for patients; about 5% of the population would experience claustrophobia in the environment in which MRI scans are conducted. For this reason, some patients are sedated prior to the process.
MRI’s are entirely safe however ferromagnetic implants may torque, causing damage to vessels and may even be fatal. This is why all healthcare personnel as well as patients have to be screened and thoroughly educated to prevent such disastrous incidents as the magnet is always switched ‘on’.
Apart from that risk, the only other negative point about MRI scans is that they require more patient cooperation than CT scans.
CT scans are best used for the evaluation of any acute changes in mental status, acute trauma to the spine and brain, focal neurologic feelings, suspected subarachnoid haemorrhage, as well as conductive hearing loss.
CT scans are very safe, fast, and reliable. However, the radiation exposure does have to be decreased when it is used on children.
Research involving these scans has shown substantial differences between the brains of people who later went on to develop psychotic symptoms and those who didn’t.
Those who went on to develop psychosis had less grey matter, specifically in the right temporal and the frontal lobe. These are the areas of the brain which are closely associated with memory, emotions, social behaviour, and attention.
Scientists have suggested that these differences, as well as others discovered in this study, may indicate an individual’s vulnerability to the development of psychosis.
Treatment
There are four different types of therapy available for individuals with psychiatric problems:
- Drugs
- Psychotherapy; this can either be for the individual alone, for a group of people affected by psychotic disorders, or for the family of a psychotic patient
- Physical treatment methods
- Behavioural modification; this uses aids such as hypnosis, relaxation, and abreaction
Physical methods have been used for the treatment of psychiatric disorders for a very long time. The first major advance was when as with most scientific advances, convulsive therapy, also known as electroplexy, was accidentally discovered in 1933. It involved the passing of an electrical discharge through the central nervous system (CNS). In 1938, this process was made less extreme when two men, Cerletti and Bini, found that introducing a small electric current across the forehead of the patient (modern electro-convulsive therapy; ECT) was just as effective.
It was a revolutionary discovery in psychiatry, as about 40 years ago, psychiatric illnesses were as dreaded as cancer is to us today. Cases and symptoms were immensely more severe as there was no way to keep the symptoms at bay; most cases went untreated and deteriorated.
It was only several years after it was introduced that anaesthetics and muscle relaxants were given to the patients. This made the treatment much more pleasant for those who desperately needed it. It soon became a very safe and effective treatment for psychotic illnesses, where the only side-effects are headaches and muscle stiffness; it came to the point where patients didn’t have to be hospitalised in order to receive the treatment.
It was noted that electroplexy was most successful in cases where the patient had depressive psychosis. It was also very effective on schizophrenics where there are extreme cases of hallucinations and delusions and other such symptoms. The quickest improvement after the use of this treatment was seen in patients with acute manic psychoses, however this was only when it was used early in the development of the illness.
Research has shown that this treatment has given significantly better results that drug therapy alone.
The same effect of ECT (the electrical discharge) can be achieved with insulin coma therapy, which has received a lot less criticism.
Other physical methods of treatment which have been used in psychiatry include leucotomy (also known as lobotomy). This is a type of psychosurgery where the connections to and from the prefrontal cortex, the anterior part of the frontal lobes of the brain responsible for complex behaviour and personality expression, are severed. It became very popular about 30-40 years ago, however it is rarely used now.
Patients who are unable to care for themselves are usually hospitalized. Recovery is possible however those with severe psychotic episodes may need to be medicated indefinitely, usually in lower doses, to control the symptoms.
Prevention
Antipsychotics are used in the treatment as well as the prevention of psychosis. They work by dampening the effects of the dopamine system so as to reduce the symptoms which appear in an individual. However, they do not always work; this may be due to the possible contribution of other neurotransmitters to the occurrence of psychosis. They include gamma amino butyric acid (GABA) and glutamate. Glutamate stimulates the brain; it plays a role in memory, thinking, as well as learning. Its levels in the nervous system are affected by stress levels and the use of drugs such as cannabis. Abnormalities in its activity are believed to have an effect on dopamine levels. GABA has the opposite effect as it slows down brain activity and also affects dopamine levels.
Psychotherapy is used a lot as a treatment in modern psychiatry; it is also being incorporated into psychosis prevention programs. It ranges from superficial psychotherapeutic counselling, where the therapists simply allows the patient to talk about their problems, to deep psychotherapy, where these problems are analysed at a further level. More recently, new techniques have been introduced where the behaviour rather than the thoughts of a patient are dealt with; these are called behaviour therapies.
Cognitive Behavioural Therapy (CBT) is most commonly used. Its purpose is to allow patients to face their problems and think about them in ways that would cause them less emotional/mental distress. It also teaches people how to cope with these problems. Studies have been conducted in recent years, and have shown a significant decrease in psychotic experiences in patients who have received the treatment, especially in the first few months of the treatment.
Evidence has shown that CBT, when given for longer durations (6 to 12 months), is more effective at reducing the effects of psychotic symptoms and helping with recovery (as well as prevention) than when provided for shorter periods of time (less than 3 months).
CBT seems to be a reasonable choice for a method of prevention as the majority of people who are at risk of developing psychosis would have had distressing or disturbing experiences which would have given rise to the disorder. CBT would give individuals the ability to find explanation for these experiences and it would help them deal with them so that they do not cause enough distress in their lives to trigger the development of psychosis.
Research is being conducted to improve and develop CBT to reduce the risk of triggering psychosis and other psychiatric disorders in susceptible individuals. There are also many clinical trials underway testing the extent to which CBT contributes to the prevention of psychosis, with as well as without low doses of antipsychotic drugs. The results so far have shown that there is a considerable delay in the occurrence of the disorder in those who receive those treatments.
There is no known way to actually prevent psychosis however early treatment of first-episode psychosis -the first time that psychotic symptoms are experienced by an individual to whom they would seem unfamiliar and frightening causing confusion and even distress -seems to help reduce the disruption a disorder can cause in a person’s life.
This theory was confirmed by a reduced response shown by psychotic patients who were treated later in their illness in the 10-year follow-up of the early Treatment and Intervention in Psychosis (TIPS) study in Denmark and Norway. By the end of the 10 year period, a higher percentage of the patients who were treated at an early stage recovered.
The study was very selective, only severely impaired patients were used because they were thought to produce better and clearer results than patients who weren’t as badly affected by the disorder.
Patients who were treated at an earlier stage were more likely to have fully recovered by the end of the 10-year period.
Although it is possible that the results of this experiment were due to chance, the correlation is strong and it is very likely that the time of intervention is related to the rate of recovery.
In order to prevent psychosis altogether, one would have to be able to identify those who are at a higher risk of developing the disorder. There have been major developments in this ability over the last 15 to 20 years.
There are many methods by which we can theoretically prevent the development of the disorder, most of which are the different treatments which are given to those who have psychosis.
A recent analysis has shown that the number of individuals with psychosis would decrease by 33% if childhood adversity was completely removed from the population. This means that supporting projects against child adversity in turn helps with the prevention of psychosis. This method of prevention could potentially be used for most of the environmental factors which are linked to the development of psychosis.
The recent study ‘Early detection and intervention evaluation for people at risk of psychosis,’ also investigated the idea of preventing psychosis in adults who are more susceptible to it.
Two years into after the start of the treatment, 2% fewer individuals who received it went on to be diagnosed with psychosis than those who did not receive any form of treatment.
According to Robin Murray, professor of Psychiatric Research at the Institute of Psychiatry, King’s College London, it is not yet possible to prevent psychosis. However, if everybody in UK stopped smoking cannabis we could prevent about 15% of the number of cases of psychosis (R. Murray, personal communication, March 23, 2013).
The results of all these studies and research are promising as to the future of the prevention of the disorder. However, it will probably be many years before we are able to completely prevent the occurrence of psychosis in susceptible individuals as a lot more funding and research needs to be conducted to better understand its causes of the disorder, how to better detect those who are likely to develop it, and which methods of prevention are most likely to prevent it from ever occurring.
Related

Tapeworm Symptoms, Treatment, And Prevention

Misconceptions of Mental Illness, Facts You Should Know

Breaking the Stigma: My Journey with Trichotillomania and a Hypothetical Psychiatric Diagnosis That Changed Everything

The Digestive Tract and Parkinson's Disease: A Possible Link

Parkinson’s Disease - What’s New?


")