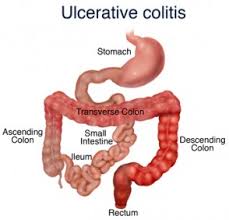
Managing Ulcerative Colitis

Case ONE: 71 year old Mrs Wretched; Extensive Ulcerative Colitis (20 years history)
Here are the problems:
- Slightly low K+
- Low Albumin (may suggest nephrotic syndrome, hepatic cirrhosis, CHF, Malnutrition, Acute and chronic inflammatory responses)
- Low Hb (due to bleeding; address anemia?)
- Comorbidities: CHF, Mild Dementia, Depression, Osteoarthritis
- Elderly
Usually in failed ASA therapy (e.g. sulfasalazine), Immunosuppressive agents (e.g. azathioprine, mercaptopurine, methotrexate or cyclosporine are used.[1] Azathioprine and mercaptopurine are effective long term.[1] Other treatment options include Pentasa SR (mesalazine) 2-4g/day (bioavailability in colon =59%).[1]
Elderly are more prone to steroid adverse effects and these include cataracts, fractures and delirium which is problematic for Mrs Wretched. [2] Oral Budesonide can be used instead for mild to moderate UC because of its limited systemic absorption but she should be monitored for delirium, hypertension, osteoporosis and diabetes.[2] Those older than 65 years have increase susceptibility of virulent Clostridium Difficile strain infection that leads to prolonged hospitalization.[2] They are also at increased risk of demyelinating disease, malnutrition and require blood transfusions once hospitalized as well as have a higher inpatient mortality rate.[2]
Initial Management Plan
- Address her low Hb levels & correcting underlying anemia from blood loss
- Address cause of bleeding (has aspirin/clopidogrel been used for longer than 12 months, perhaps need to just be maintained on clopidogrel only plus increased anticoagulation effects of aspirin and sulfasalazine)
- Is sulfasalazine causing nephrotoxicity hence low albumin and higher creatinine?
- Rule out malignancies
- Address slightly low potassium levels, perhaps due to bleeding and/or malnutrition?
- Address malnutrition
- Address possible infection and treat if necessary short term with monitoring for advere events
- Rule out Clostridium difficile before oral Cyclosporin use
- More than 6 bloody bowel motions indicating acute severe UC hence indicating need for I.V. high dose corticosteroids (hydrocortisone 400mg/day or methylprednisonolne 60mg/day) to induce remission despite corticosteroid adverse events risk in elderly [2]
Though more studies in patient over 55 years old are needed, Integrin receptor-antagonists especially Vedolizumab proved to be safer versus Natalizumab (GEMINI 1 &II trials)and are recommended as first-line therapy for moderate to severe UC and preferable over anti-TNF- α in elderly.[2]
Standard management of UC involved the stepwise approach of mesalazine, corticosteroids and immunomodulators or surgery.[3]Tacrolimus (immunosuppressant) and Anti-tumor necrosis factor (TNF) agents are safe and effective as part of the UC-treatment management of moderate to severe UC.[3]
Mrs Wretched should be given blood transfusion to correct her low Hb and electrolyte disturbances. I suggest that sulfasalazine be ceased and review Aspirin use and consider ceasing aspirin and she be continued on clopidogrel alone due to added drug interactions with potential treatments with NSAIDs. Lab monitoring of bloodwork is vital. Ensure she gets adequate nutrition. ) Commence antibiotics (ciprofloxacin and metronidazole) if infection present and Clostridium difficile has been ruled out.
Failure of medical management may indicate Mrs Wretched for surgery especially since UC has been present for greater than 7 years. Early elective surgery provides better prognosis than emergency surgery thus timely surgery in elderly are warranted when needed.[2] Optimized disease management pre-surgery like decreasing steroid exposure, improving nutritional status and peri-operative management of comorbidites like hypertension and diabetes are vital in improving the healing process and decrease morbidity/mortality risks.[2] However, there’s an increased risk of increased stool frequency and fecal incontinence with IPAA (Ileal pouch-anal anastomosis) surgery.[2] Urgent surgery in UC is indicated here due to uncontrolled colonic bleeding, medical management failure and elective surgery indications include long term steroid use, dysplasia or adnocarcinoma and presence of disease for 7 to 10 years but overall risks and benefits have to first be weighed out in her case due to anticoagulant use and her other comorbidities. [2]
Higher creatinine levels (though still within normal range in this case) indicate poor clearance of creatinine by the kidneys, suggesting sulfasalazine use needs to be reviewed and replaced. Adverses events are attributed to sulfapyridine component within sulfasalazine thus mesalamine can be administered alone instead to prevent these side effects.[5] Mesalamine is however can also cause nephrotoxicity so regular monitoring is required.[1]
Taking sulfasalazine (usual first line treatment for UC) for 10 years may have caused nephrotoxicity hence the low albumin.[2] If combined with thiopurines, leukopenia can result.[2] Moreover, there’s problem of compliance due to difficult administration of ASA rectal treatments.[2] Immunomodulators like MTX should be reserved for Crohn’s disease and have drug interactions with frusemide, NSAIDs and antibiotics plus depletes folic acid.[2] Cyclosporine is rarely used due to its toxicities in all patient ages.[2]
Thiopurines increase risk of non-melanoma skin cancers by two-fold even after discontinuation , increases lymphoma and acute pancreatitis occurs within first few weeks in 3% of patients (according to meta-analyses) and have greater impact on morbidity and mortality in the elderly.[2] Elderly are suggested to use biologics and/colectomy instead.[2]
A retrospective observational study showed that tacrolimus and anti-TNF agents are safe and efficacious in moderate to severe UC although more randomized controlled trials are still needed.[4]




Anti-TNF-α agents (e.g infliximab) modestly increase susceptibility to infection (TB, Hepatitis B and endemic fungal infections;TB risk studied from a recent multicenter retrospective longitudinal cohort study) and with sub-optimal efficacy but increased adverse events especially in the elderly >65 years old.[2] Combination with biologics further increase infection risk due to increased immunosuppression without additional benefit (e.g. did not decrease risk of new or recurrent cancers in IBD according to CESAME trial) .[2] Increased malignancy risk (lymphoma and melanoma) are observed.[2] Furthermore, even though highly effective for moderate to severe UC and CD, it should be avoided in Mrs Wretched due to her CHF (especially if it is advanced).[2] Careful consideration of risk versus benefits and choosing the right immunomodulator and ease of use are pertinent.[2] Immunomodulators should be considered to be ceased and patient be maintained on continued biologic monotherapy if low relapse risk to decrease malignancy and opportunistic infection risks.[2]
Antibiotics like Ciprofloxacin and Metronidazole are indicated for mild-moderate disease.[2] However, ciprofloxacin is associated with inceased clostridium difficile risk and decrease seizure threshold.[2] Metronidazole can lead to peripheral neuropathy which causes additional problems in the elderly along with adverses effects like anorexia and nausea which can limit appetite and detrimentally affect nutritional status.[2] Any duration of use requires monitoring for adverse events.[2] Short term use are preferred.[2,5]
Part Two
I.V. Cyclosporine 4mg/kg/day is indicated if there’s no response to IV corticosteroid after 1 week.[5] If remission is achieved, she can be changed to oral prednisone 40 to 60mg/day (short term) and Vedolizumab (300mg I.V. on weeks 2 and 6 then every 8 weeks) be commenced to withdraw steroid use and consider recommencing on aminosalicylates like mesalamine 2.4 to 4.8mg/day instead of sulfasalazine after 1 to 2 months when UC severity is mild to moderate.[5] Topical mesalamine preparations like suppositories or enemas (Rowasa suppositories 1g daily to three times weekly or Canasa enema 4 g daily to three times weekly) are more efficacious than oral preparations although combined topical and oral formulations are optimal and added efficacy in UC patients.[5] Oral sustained-release mesalamine preparations will have greater bioavailability to the indicated site of action than non-SR forms.[5]
REFERENCES
1) Zhang ZM, Li W, Jiang XL, Efficacy and safety of Adalimumab in Moderately to Severely Active Cases of Ulcerative Colitis: A Meta-Analysis of Published Placebo-Controlled Trials. Gut Liver 2016 Mar 10 (2):262-274. Available from : https://www.ncbi-nlm-nih-gov.ezproxy.utas.edu.au/pubmed/26780088
2) Elizabeth S. John, Kristina Katz, Mark Saxena, Sita Chokhavatia, Seymour Katz. Management of Inflammatory bowel disease in elderly.Current Treatment options in gastroenterology Sept 2016, Volume 14, Issue 3, pp285-304. Available from: https://link-springer-com.ezproxy.utas.edu.au/article/10.1007%2Fs11938-016-0099-6
3) Danese S, Colombel JF, Peyrin-Biroulet L, Rutgeerts P, Reinisch W.Review article: the role of anti-TNF in the management of ulcerative colitis -- past, present and future. Aliment Pharmacol Ther. 2013 May;37(9):855-66. doi: 10.1111/apt.12284. Epub 2013 Mar 13. Available from: https://www.ncbi.nlm.nih.gov/pubmed/23489068
4) Yamamoto T, Shimoyama T ,Umegae S, Matsumoto K.Tacrolimus vs. anti-tumour necrosis factor agents for moderately to severely active ulcerative colitis: a retrospective observational study. Aliment Pharmacol Ther. 2016 Mar;43(6):705-16. doi: 10.1111/apt.13531. Epub 2016 Jan 13.Available from: https://www-ncbi-nlm-nih-gov.ezproxy.utas.edu.au/pubmed/26762838
5) Joseph T.DiPiro, Robert L.Talbert et al. Pharmacotherpy-A pathophysiological approach 10th Edition. McGraw Hill. New York. Chapter 34







