Benchmarking Child Growth From Infant to Adolescent with Specific Signs


Growing Child

General Patterns of Development
Child’s growth is one of the best thing you can observe and enjoy being a caregiver. A complete child development encompasses its physical, biological and emotional growth. As a parent we always want a benchmark or anxious about how well our child is growing? Here in this article we can easily find and spot or child growth and development pattern.
Growth and development are marked by relatively predictable events. To understand the events related to this process, the patterns of development and the sequencing and rate of growth must be considered.
Growth and development occur in regular related patterns.
- Each system has critical periods of development.
- Each is reflective of physical development and maturation of neuromuscular function.
- The directions are:
Cephalocaudal
- development begins at the head
- the head is large and complex and the lower end is simpler and develops later
Proximodistal
- "near-to-far" concept or "midline-to-proximodistal" concept
- CNS develops prior to peripheral nerves
Differentiation
- simple occurs first and is followed by complex (i.e., the child rolls over, crawls, creeps, stands, walks, and finally runs)
- broad global behaviors are followed by more specific and refined behaviors (i.e., an infant will "palm" an object while trying to pick it up before being able to use the thumb and forefinger in a "pincer" grasp to pick up a small object)
Brain Development


Sequencing and Rating Growth
- There is a predictable sequence for all dimensions of growth.
- Each stage is affected by all preceding and following stages.
- Does not occur at the same rate for all children.
Factors adversely affecting growth and development:
- Genetic Factors
- Physical Factors
- Environmental Factors
- Social, Cultural and Affective Factors
Each Phases of Development
NEONATES (Birth - 1 month)
General Considerations
- Major stressor - physical immaturity.
- Remember - limited cerebral cortical pathway - connections not fully established
- Behavior is largely reflex in nature
Physical Considerations
- Position is one of flexion
- Metabolic rate about 2 times adult's with body surface area 3 times adult's - therefore, predisposed to excessive heat loss
- Also have difficulty in dissipating extra heat - therefore, risk of hyperthermia
- Greater risk for acidosis due to high metabolic rate
- Rate of fluid exchange twice that of adult with greater percentage of extracellular fluid
- Immature kidneys can't concentrate urine - therefore, higher risk for overhydration
- Head is 70% of eventual body size
- Skeletal system contains large amounts of cartilage. Fontanelles are open because six skull bones are soft and not yet joined.
- Eyes can detect movement, colors, changes in brightness, and visual patterns
- Hears very well - knows mother's voice by 3 days of age
- Has well developed sense of smell and can recognize caregivers by smell
Psychosocial Considerations
- Major developmental task is bonding with primary care giver
- Development of trust essential during this period
Safety Issues at this Age
- Obligatory nose breather
- Vulnerable to aspiration due to proximity of respiratory & GI passages, immature cardiac sphincter, small stomach capacity
- Vulnerable to temperature changes due to inability to sweat in response to heat and shiver in response to cold
- Substantial fluid losses may occur from nose breathing, insensible losses through skin, limited ability to concentrate urine, warm environment, fever, GI losses, high metabolic rate
- Limited inflammatory response and antibody production caused by immature immune and liver functions
Interventions to Promote Growth and Development
- Touch and motion are essential to normal growth and development
- Promote the idea of the infant as an individual with unique behavioral characteristics
- Swaddling promotes sleep and maintains body temperature
- Intermittent, vertical rocking promotes bright-alert behavior, while continuous horizontal rocking induces more drowsy behavior.
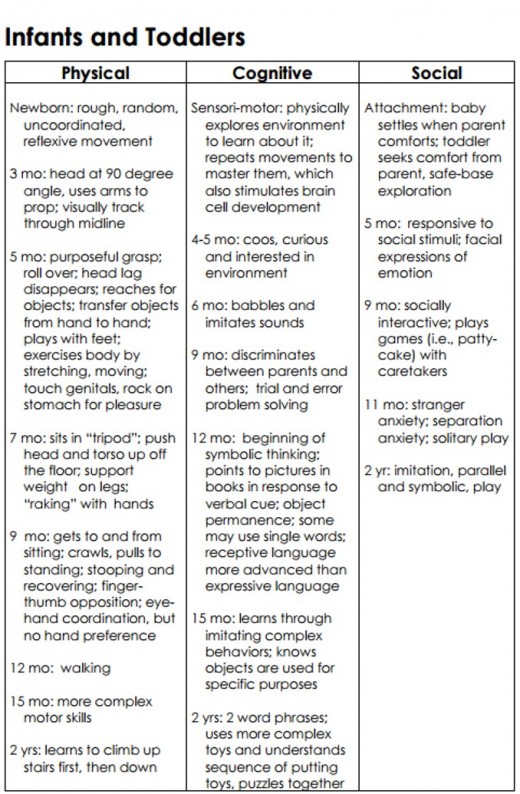
INFANTS (1 month - 12 months)
General Considerations:
- Time of rapid growth and development
- Changing physically and socially and learning about the environment
Physical Considerations
- Growth is very rapid, particularly during the first 6 months of life
- Birth weight has doubled by 5 months and tripled by 1 year
- Length has increased by 50% by 1 year of age
- Head circumference increases by 33% by 1 year of age
- Brain weight has increased two and a half times by 1 year of age
- Visual acuity increases from about 20/100 to 20/40
- Vital signs change - heart and respiratory rates slow and blood pressure increases
- Thermoregulation becomes more efficient and increased adipose tissue is laid down by 6 months to provide insulation
- Continues to have a greater proportion of extracellular fluid (ECF)
- Digestion is maturing, but solids may still pass through undigested
- Tongue becomes smaller in relation to rest of oropharynx and mature swallow reflex develops. Extrusion (tongue thrust) reflex fading by 4 months of age.
- Teeth develop (number of teeth expected is figured by taking the age of the child - 6. In other words, a 9 month old child would be expected to have 3 teeth [9 - 6 = 3])
- Fine motor development:
- Can voluntarily grasp an object by 5 months
- Can hold bottle and feed self a cracker by 6 months
- Can transfer objects from one hand to the other by 7 months
- Neat pincer grasp in place by 11 months
Gross Motor development
- Can lift the head and front portion of chest approximately 90 degrees by 4 months
- Has well established head control by 6 months
- Rolls from abdomen to back purposefully by 5 months and from back to abdomen by 6 months
- Sits alone by 7 months using hands for support; sits unsupported by 8 months
- Crawls (moving forward with belly on floor) by 6 - 7 months
- Creeps (moving forward with belly off floor) by 9 months
- Pulls into standing position by 9 months
- Walks supported by hand holding or by hanging on to furniture by 11 months
- Walks with one hand held by 1 year and may walk unsupported by this time
Psychosocial Considerations
- Bonding with parents requires touching, talking, and playing
- Needs to develop intrafamily relationships with siblings, grandparents
- Responds more to mother than others, but continues to respond to "mothers" whether familiar or no at 8 - 12 weeks
- Show preference for mother at 6 months of age
- Begin to show attachment to other family members about 1 month after beginning to show attachment to mother
- Begin to protest when mother leaves at about 6 months (although may not notice at first if involved in play)
- Begin to protest mother leaving before she leaves by 11 - 12 months
- Stranger anxiety develops between 6 and 8 months
- Stressors: loud noises, bright lights, sudden environmental changes
- Cognitive abilities depend on age in months
- Reactions move from reflexive to intentional
- Language development:
- vocalizes by 5 - 6 weeks
- makes single vowel sounds by 2
- makes some consonant sounds, coos, gurgles, and laughs out loud by 3 to 4 months
- imitates sounds and makes additional consonant sounds by 8 months
- understands the meaning of words (including "no") and follows simple commands by 10 - 11 months of age
- can say 3 - 5 words by one year
- By 8 months the infant begins to coordinate two or more actions
14. Can play simple games by 6 months, imitate actions and noise by 7 months, imitate sounds by 8 months, and play pat-a-cake and peekaboo by 10 months
Safety Issues at this Age
- Vulnerable to URIs and aspiration due to small airways, limited ability to chew, proximity of respiratory and GI passages, immature cardiac sphincter, and small capacity of stomach
- Greater proportion of ECF and continued immaturity of renal structures places infant at continued risk for dehydration
- Respiratory failure possible because of poorly developed accessory muscles of respiration and limited diaphragmatic excursion
- Unable to distinguish dangers
- Aspiration is the leading cause of fatal injury in children < 1 year
- Motor vehicle injuries are the leading cause of accidental death in children < 1 year
- Other risks include suffocation, poisoning, burns, drowning, and other bodily damage
- Keep siderails up at all times
- Have bulb syringe available for suctioning
Interventions May Needed
- Major fear: separation from primary caregiver
- Parental anxiety may be transmitted to child
- Mistrust may be evidenced as failure to thrive
- To decrease anxiety:
- allow child to keep parents in line of vision
- have familiar objects available
- cuddle and hug the infant
- distractions such as pacifiers, bottles, and toys may help when assessments and interventions are performed
- The greater the lack of harmony between the child's temperament and the parent's ability to deal with it, the greater the risk for parent-child conflicts (Whaley and Wong, 1995).
- Stranger anxiety may be lessened by talking softly, meeting the child on his/her level, maintaining a safe distance, and avoiding sudden gestures or sounds.
- Anticipatory guidance including immunizations, injury prevention, and strategies to promote growth and development should be discussed with families
- When teaching procedures to parents, provide opportunities for return demonstration

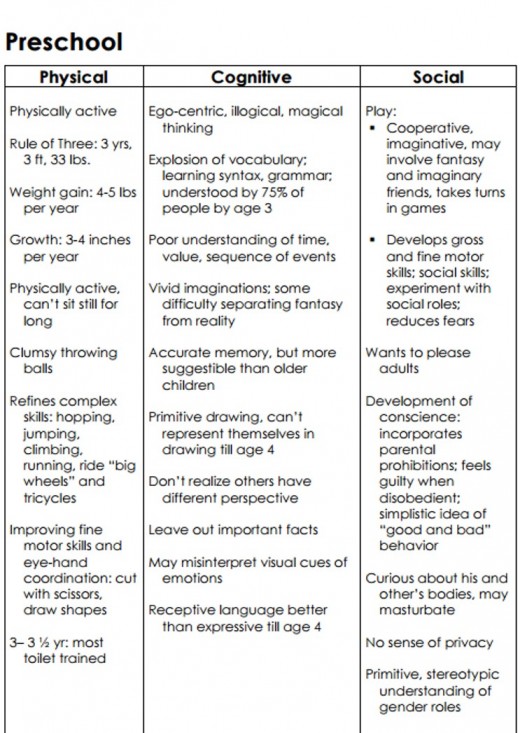
PRESCHOOLERS (3 - 6 years)
General Considerations
Considered critical for emotional and psychological development
Physical Considerations
- Weight gain is about 2.3 (5 lbs.)/year and height increases by about 2.5 - 3 inches/year
- Gross and fine motor skills continue to develop
- Body systems are mature
Psychosocial Considerations
- Learning to play in groups
- Major fears: fear of the unknown, of the dark, of mutilation, bodily injury, of being left alone
- May perceive procedures as mutilation or as punishment
- Able to tolerate brief separation from parents with little protest if given explanations of where parents are and when they will return
- May have difficulty differentiating reality from fantasy but moving toward understanding of cause and effect
- Verbal expressions of pain and discomforts not always reliable
- Critical period for speech development occurs between 2 and 4 years.
- Failure to master results in stuttering or stammering
Interventions to promote Growth and Development
- Explain procedures (be honest) and unfamiliar objects
- Demonstrate use of equipment, let child play with the equipment if possible/safe
- Use of dolls/puppets for explanations when performing procedures may alleviate anxiety
- Involve the child whenever possible
- Provide rest periods during long procedures, testing, therapy
- Assess and manage pain (distractions may help for short term pain during a procedure)
- Allow child to choose site for an injection
- Offer stickers or other rewards for cooperation
Do not restrict child's movement, unless necessary for safety reasons
TODDLERS (1 - 3 years)
General Considerations
- Slowed physical growth but continued systems maturation
- Striving for independence and self-assertion
Physical Considerations
- Birth weight quadrupled by 2 1/2 years of age
- Average weight gain is 1.8 - 2.7 kg/year
- Average height at 2 years is 86.6 cm (34 inches) and is about half of adult height
- Height increases about 3 inches/year and is mainly seen in the lengthening of legs
- Head circumference increases about 2.5 cm in 2nd year then slows to about 1.25 cm/year by 5 years. Head and chest are approximately equal in size until after second year.
- Visual acuity is about 20/20 and other senses are well developed
- Respiratory and heart rates slow and blood pressure rises
- Begins to have some control over elimination processes
- Major gross motor skill is development of locomotion
- Major fine motor skill is increased manual dexterity
Psychosocial Considerations
- Giving up dependence in exchange for control, independence, autonomy
- May attempt to exert control through negativism
- Has rapid mood swings
- Becomes verbal
- Tolerates separation from parent/caregiver
- Interacts with others in a decreasingly egocentric manner and begins to act in a "socially acceptable" way
- Acts in a ritualistic manner, which provides comfort
- Engages in parallel play (plays alongside other children but not with them)
Safety Issues
- Injury is the leading cause of death
- Motor Vechcle Accident's cause of most accidental deaths followed by drowning, burns, poisoning, and aspiration/suffocation
- High risk for dental caries (nursing caries) if continuing to drink from bottle
Interventions to promote Growth and Development
- Any invasive procedure (even no painful) may evoke an exaggerated avoidance response
- Hospital environment, strangers and procedures may evoke terror response
- Separation anxiety may be intense
- Short attention span and limited memory capability
- Magical thinking may lead to perceiving machines as "monsters" or to feeling responsible for illness
- Tend to falsely reason that when any two events occur together, that one has caused the other
- Behavior can be very ritualistic; upset by changes in environment and daily activities
- Low tolerance for frustration or pain; exaggerated responses to both
- Responds better to visual then spoken cues
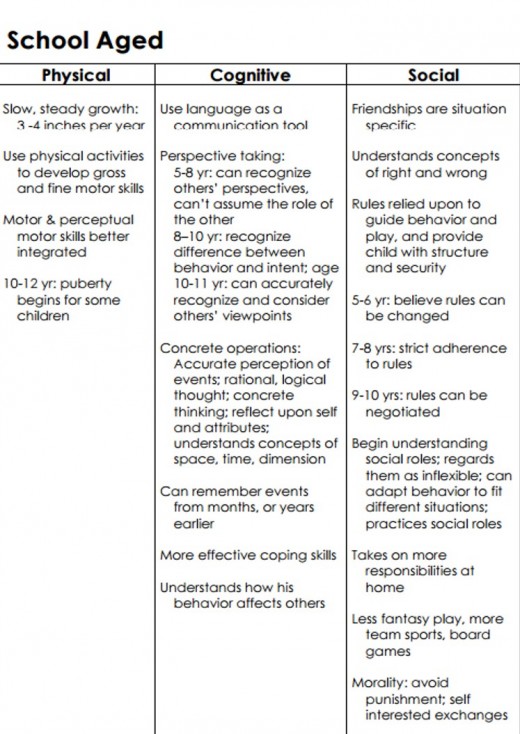
SCHOOL-AGE CHILDREN (6 - 12 years)
General Considerations
- Great social and cognitive change
- Maturation from biological and physiological standpoints
- Gross motor skills organized and purposeful
- Exhibit competition, learning styles, and great sense of humor
Physical Considerations
- Grows about 2 inches/year and will double weight by age 12 years
- Girls surpass boys in both height and weight by end of this period. Growth spurt for girls begins about 10 years and boys about 2 years later
- Become slimmer with lower center of gravity. Fat decreases and muscle mass increases.
- Will loose all primary teeth during this period
- Enters prepubescence during the last 2 years
- Gross and fine motor ability and coordination increase
Psychosocial Considerations
- Decrease in egocentricity
- Prefers socializing with peers and friends vs. family
- Wants some control over privacy
- Can be reasoned with - increased concept of right and wrong
- Likes reward systems
- Great fears of the unknown: of bodily injury, mutilation, separation, death
- May perceive hospital treatments as punishments
- Can reason systematically about tangible or familiar objects and use logic to analyze relationships and implications of events
- Able to describe discomforts in some detail
- May have little understanding of anatomy, body functions, and illness
Safety
- Ideal time to begin to be responsible for own health
- Begin to engage in risk taking behavior
- Major sources if accidental injuries include MVA, bicycles, skateboards, and skates
- Injury prevention directed toward education as well as provision of safe play areas
Interventions to promote Growth and Development
- Explain procedure in advance, use correct terminology
- Explain equipment, let child touch equipment and try it out if safe
- Allow child to have some control, offer choices if possible provide privacy
- Assess and manage pain; may understand the use of a PCA or parent
- May control analgesia; schedule medication to prevent pain (may need around-the-clock meds)
- Assess response to pain medication prior to and after each dose to be sure patient is receiving enough to control pain
- Define and reinforce behavior limits; use visual aids; be concrete and specific
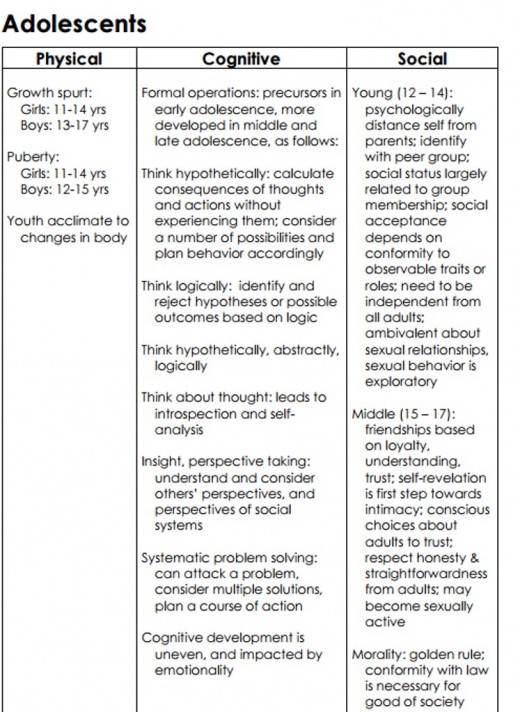
ADOLESCENTS (12 - 18 years)
General Considerations
- Longest period of development - becoming more "adult"
- May have great change and turmoil
- Characterized by biologic, cognitive, psychological, and social change
Physical Considerations
- Biological changes constitute period called puberty
- Become sexually mature as well as fertile
- Final 20 - 25% of linear growth achieved and up to 50% of ideal body weight is gained
- Lean body mass increases in both sexes and fat mass increases in girls but declines in boys
- Neural system continues maturation as reflected in increased cognitive abilities
- Skeletal growth is faster than muscle growth, thus allowing for incoordination
Psychosocial Considerations
- Move from concrete thinking to abstract, hypothetical type thinking
- Separating themselves from parents and other authority figures and relationships with peers become more important
- Body image: may be extremely self conscious with body changes, appearance, perceived flaws
- Behavior may be inconsistent, unpredictable, moody, regressive; strongly influenced by peers
- May be hypersensitive/hyperreactive to pain
- Need time to adjust and cope with events
- May need but not request adult support to cope effectively
- Develop ability to think more abstractly, deductively, and to form their own opinions
Safety
- Risk taking behavior is common
- Accidents are the single greatest cause of death
- Car accident cause approximately 2/3 of all accidental deaths and alcohol is involved in the majority of these
- Homicide is the second leading cause of death and first for black adolescents. Firearms are involved in > 70% of homicides.
- Suicide is 3rd most frequent cause of death in this age group
Interventions to promote Growth and Development
- Discuss sensitive issues (such as sexuality) in private
- Explain procedures and supplement with reasons
- Privacy is very important
- Involve patient in planning and decision making as much as possible
- Allow adolescent to maintain as much control as possible
- Provide essential teaching based on how the individual learns the best (auditory, visual, etc)
- Provide information on pain control methods, assessment scale, schedule for pain management, need to ask for pain medication as soon as pain starts, need for them to provide information on degree of pain relief

")


