Achalasia Of The Cardia Health Implication: The Story Of Guadalupe Santiago From Bolivia

Achalasia Of the Cardia

Barium Swallow Diagnostics To show Achalasia

The Story Of Guadalupe Santiago From Bolivia
Guadalupe is a post graduate student of Economics in Bolivia. For the past few weeks she has been experiencing difficulty in swallowing which comes with pain. Even after taking some over-the counter medication, the symptoms still persisted but in a mild occurrence. Some days ago, she started experiencing chest tightening which continued until it exacebated to vomiting of undigested food accompanied by a rotten smell and cough. She was rushed to the hospital and after some procedures, was diagnosed with Achalasia of the Cardia, Stage III.What exactly are we talking about here?
Pathophysiology
The histo-pathology of Achalasia involves inflammation of the myenteric plexus of the Oesophagus with diminution of ganglion cells. Significant reduction in nitric oxide synthase containing neurons has been demonstrated using immuno-histochemical staining.
Lower Oesophageal Sphincter pressure and relaxation are controlled by excitatory substances such as acetylcholine and inhibitory substances such as nitric oxide, vasoactive intestinal peptide etc. Persons with Achalasia lack non-cholinergic and inhibitory ganglionic cells and non-adrenegic cells hence causing an excitatory and inhibitory inbalance in neurotransmission. When this occurs, a hypertensive non-relaxed Oesophageal Sphincter results.
Classification
As the disease progresses, the spasm of the Lower Oesophageal Sphincter causes increase pressure within the Oesophagus (intra-Oesophageal pressure), thereby expanding the diameter of the Oesophagus. This leads to graduation dilation which continues as the disease progresses. As this happens, the Oesophageal mucosa can be irritated and inflamed. Such inflammation can cause minute lesions/injury to it. During recovery of such injury, scar is formed. In later stages of the disease, such scar formation will result to erosive changes of the musoca of Oesophagus with considerable dilatation with sigmoid-shaped elongation. So, we can summarize its stages or classification into 4:
- Functional spasm without Oesophageal dilation
- Constant spasm with a moderate Oesophageal dilation and maintained peristalsis.
- Cicatrical changes (Changes associated with scar formation which remained after the development of a new tissue over a recovering wound or sore) of the wall with expressed Oesophageal dilation, the peristalsis is absent.
- Considerable Oesophageal dilation with sigmoid-shaped elongation and the presence of erosive changes of Oesophageal mucosa.
What Is Achalasia of the Cardia
Achalasia means "Failure to relax"; hence Achalasia of the Cardia is the disease characterized by failure of the lower Oesophageal sphincter to relax when swallowing. Normal Peristalsis is interrupted and food cannot enter the stomach. This Lower Oesophageal Sphincter is near the junction between the Oesophagus and the upper part of the stomach (called the Cardia) and hence the name.
Peristalsis is a radially symmetrical contraction and relaxation of muscles which propagates in a wave down a muscular tube in an antegrade fashion. In the case of the Oesophagus, this aids in the movement of food in one direction downwards to the stomach. Lack of relaxation only means the Oesophageal Sphincter remains contracted. Continuous contraction is what is known as Spasm.
Causes
Cause is unknown, but there are causes believed to be behind this disease such as:
- psycho-emotional trauma
- disturbance of the autonomic nervous system
- gastroesophageal junction obstruction
- viral infection
- genetic inheritance
- autonomic diseases
Symptoms
1. difficulty in swallowing (Dysphagia). The majority of patients with such a symptom better swallow warm or hot food.
2. Oesophageal vomiting (regurgitation): Mostly, this occurs when there is an accumulation of 2 or more liters of fluid in the Oesophagus. This can occur during or immediately after meal and sometimes pain sensation is felt in advanced stages. It is accompanied with a rotten smell (Just as in the case of Guadalupe). It can also occur during sleep and hence the symptom: 'Wet Pillow'
3. Nocturnal cough: Happens as a result of fluid aspiration from Oesophagus into Trachea. For this reason, patients should sleep in a sedentary position.
4. Pain and sense of tightness in Chest (just as in Guadalupe's situation) occurs due to spasm and Oesophageal distension with the development of Oesophagitis. This pain wears a burning character.
5. Loss of weight due to prolonged disturbed food intake.
Mechanism


The Doctor's Findings
Diagnosis
- Barium Swallow
- Oesophagogastroscopy
- Chest X-ray
- Endoscopic Ultrasound
- Oesophageal Manometry
The best which confirms diagnosis is the Barium Swallow roentgenological procedure. In the beginning of the disease, an inappreciable Oesophageal dilation and temporary delay of barium above the level of the inferior Oesophageal Sphincter is revealed.
In advanced stages, considerable Oesophageal dilation and elongation with a long delay of barium are revealed. Not only that, contours of a distal constricted part of Oesophagus described as the "rat tail" or "bird beak" sign without filling defects are revealed.
Endoscopic procedure reveals erosive changes of Oesophageal mucosa and enables to take a biopsy to race out malignancy. Frequently, in advanced stages, the endoscope fails to pass through the constricted part of the Oesophagus and Cardia.
Differential Diagnosis
- Cancer of the lower part of Oesophagus and Cardial part of stomach: In cancer, irregular contours of constricted part of Oesophagus with filling defects are revealed in X-ray.
- Diaphragmatic Hypotonia: Here, high standing of the Left dome of diaphragm is revealed in the chest X-radiography.
- Pneumothorax: Absent Lung patterns on roentgenograms.
Complications
- Bleeding: Can arise owing to erosive Oesophagitis at long duration of the disease.
- Malignancy: Due to elongated (Chronic) Character of the disease.
- Pneumonia, abscesses, bronchiectasis, atelectases and Penumosclerosis due to decreasing pulmonary excursion which results from compression by dilated Oesophagus.
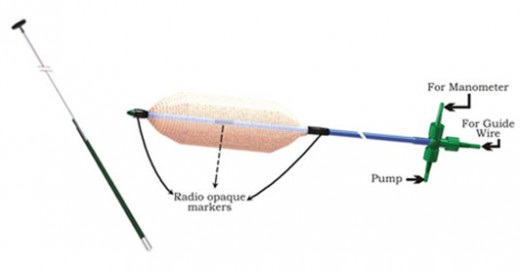
Disposable Achalasia Cardia Balloon Dilator
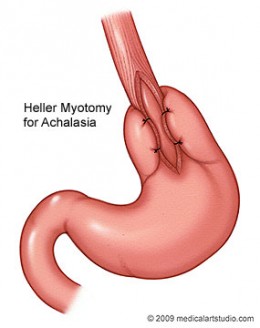
heller-myotomy
TREATMENT
1. Diet: Food should be semi-soft, without pungent relishes, chemically inactive and enriched with proteins, fats, carbohydrates and vitamins.
2. Drug Therapy: Should include local anesthetics, spasmolytics and sedative drugs. Atropic and other anti-cholinergic agents only increase the spasm of a cardial Sphincter, thus their usuage is undesirable. Drug therapy only results in temporary relief. Calcium channel blockers such as Nifedipine reduce lower Oesophageal Sphincter pressure and hence useful. Others are Nitrates such as Dinitrate, Nitroglycerin and isosorbide. But such drugs manifests into bad side effects like swollen feets and headache and stop been effective after some months, hence not recommended.
3. For patients who cannot risk surgery such as unhealthy individuals or the elderly, Botox injections are recommended. Botox is Botulinum toxin which paralyses the muscle holding the lower Oesophageal Sphincter. This lasts for 6 months but is a contra-indication for a later procedure (Heller myotomy) which is an effective surgical tactic for this illness.
4. Cardiodilatation/Pneumatic dilatation: Is indicated in I-II stage of Achalasia. It is one of the chief methods of the treatment of this pathology. The treatment is performed as follows: Under local Anesthesia by aerosol or solution of anesthetic agent (Lidocain, trimecain) through constricted part of the part of the Cardia under roentgenological check. Cardiodilator (metal, Pneumatic) is passed. The air is pumped up in balloon making pressure 200-350 mm H20. Repeated procedure is performed in 2-3 days. The course of dilation includes 3-10 procedures, depending on obtained effect.
5. Surgical
(a) Heller's Method (Oesophagomyotomy):
stages
- Cardiomyotoma
- Peritonization by gastric fundus
- peritonization by great omentum
- peritonization by diaphragmatic flap
(b)Helerovsky's method
(c) Pneumatic dilatation
There is no behavioral pattern which can be advised in order to avoid such an ailment. Nevertheless, the only advice here is: If you start having any of these symptoms: the feeling of chest tightness, cough, difficulty in swallowing and even vomiting, ensure that you see the doctor immediately.



")
