Cervical Spondylotic Myelopathy – Treatment – Physiotherapy Management


Introduction
The treatment for Cervical Spondylotic Myelopathy aims at –
- Treating the cause for the condition.
- Reducing or relieving the pain.
- Strengthening the weak muscles.
- Reducing the spasm, if present.
- Maintaining the range of motion of cervical spine and the shoulders.
- Improving the impaired functions, if any.
- Correction of improper posture.
- Teach how to carry out the activities of daily living without causing further injuries that worsens the symptoms.
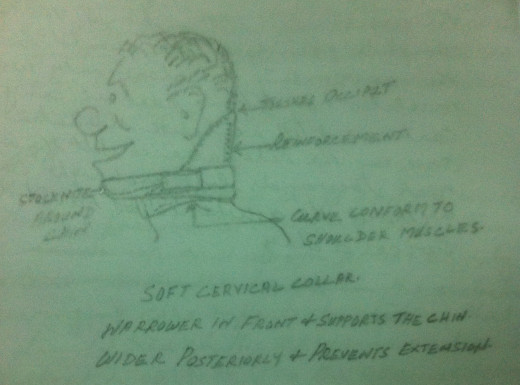
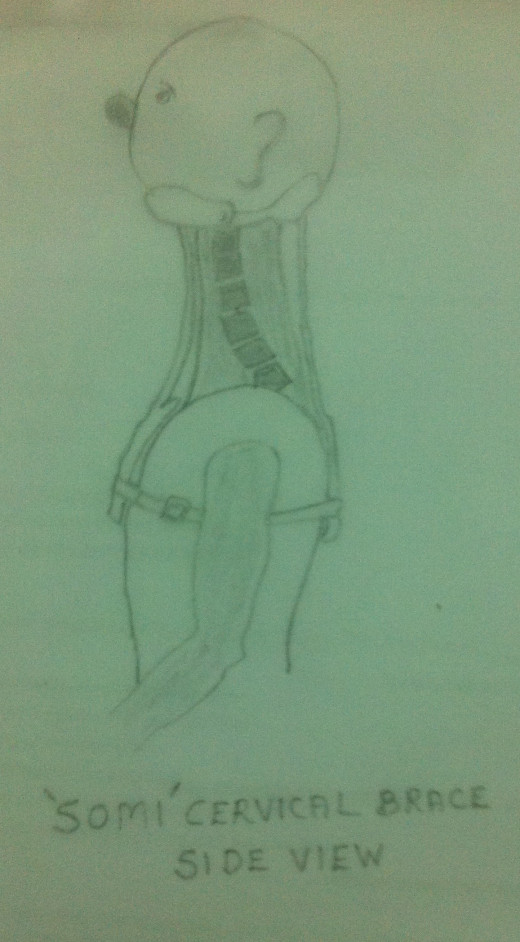
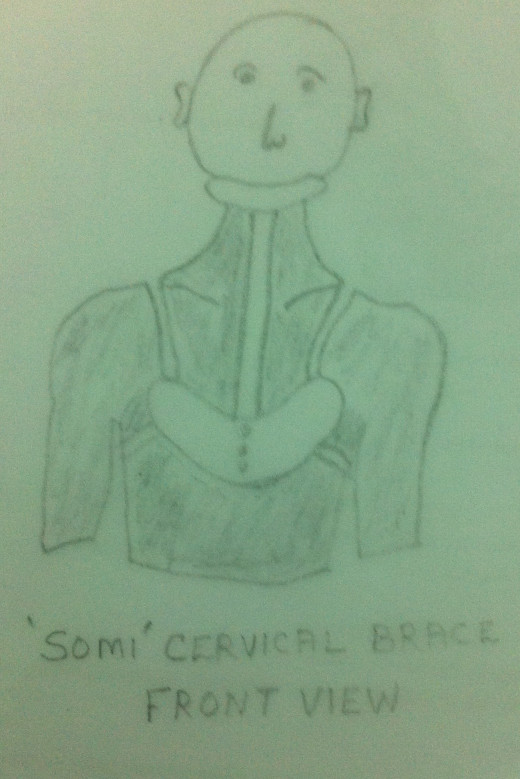
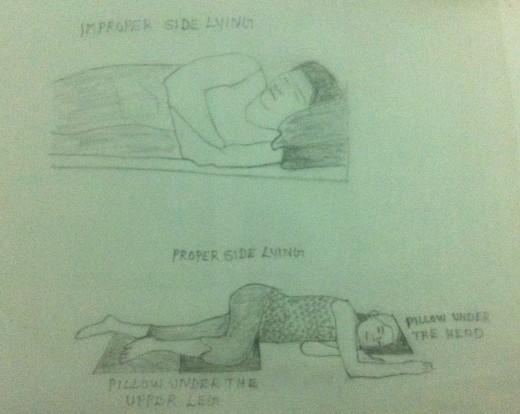
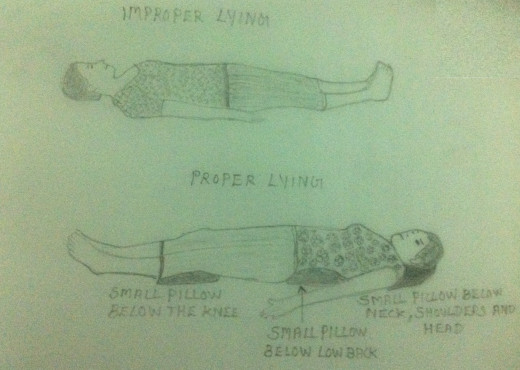
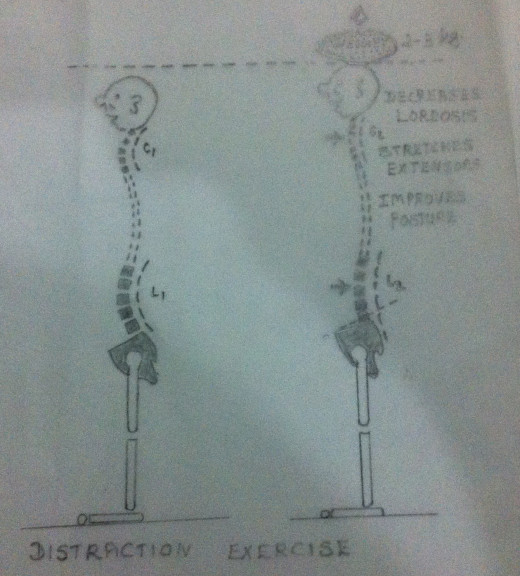
- Rest – Rest is indicated. Rest can be achieved by minimising any activity that may aggravate the symptoms. While on supine lying avoid pillows and use a small pillow while side lying so that hanging down of head may be avoided. Keeping the neck at rest will provide a certain degree of relief of symptoms. To provide rest soft cervical collar or cervical orthosis,SOMIOrthosis,may be used. Soft cervical collar is made up of felt or similar materials. The SOMI Cervical Orthosisis usually moulded with plastic and metal to conform to the portions of the head and the shoulders. It fits under the chin. The cervical collar or the orthosis provides –
- Rest to the cervical spine by restricting its movements.
- Relieves the pressure on the spinal cord or the nerve roots.
- Decreases the cervical lordosis.
- Stretches the cervical spine.
- Helps in postural correction.
But using the cervical collar or cervical brace for longer periods must be discouraged. It is to be noted that even with a few days of its use, it will become addictive and the patient will be reluctant to discard it. Prolonged use of cervical collar or brace results in the weakening of the cervical musculature and the limitation of the neck movements. Moreover using brace or collar for longer periods will enhance the process of degenerative changes in the already degenerated spine. Hence a careful and judicious use of collar or brace is advisable. If there is improvement and the symptoms have subsided the patient must be ‘weaned’ from the collar or the brace.
2. Application of Ice-Cryotherapy- If the patient is having acute pain Cryotherapy is beneficial. Due to the pain the cervical muscles may go into protective spasm which aggravates pain. Ice relieves protective muscular spasm and hence the pain. It has an anaesthetic effect also. It, to some extent, has an anti-inflammatory effect also. Prolonged application of ice is preferred.
Please refer my early article ‘The Whiplash Syndromes’ for further details.
3. Application of Heat – Once the acute stage has subsided, heat is preferred to relieve pain. Moist heat in the form of hot water fomentation to the painful areas relieves the protective muscular spasm and hence the pain. It is to be noted that even though the pain has subsided or relieved on the application of Ice or heat, they do not have any effect on the deeply situated pathological disease conditions. In the physiotherapy department superficial heating modalities like Moist Heat, Infrared Radiation etc. and deep heating modalities like Short Wave Diathermy, Ultra Sound Therapy etc. are found to be very beneficial. Laser Therapy is also found to be very useful.
Please refer my earlier article on ‘The Whiplash Syndromes’ for further details
4. Transcutaneous Electrical Nerve Stimulator (TENS) is highly beneficial to relieve the radiating pain, if present.

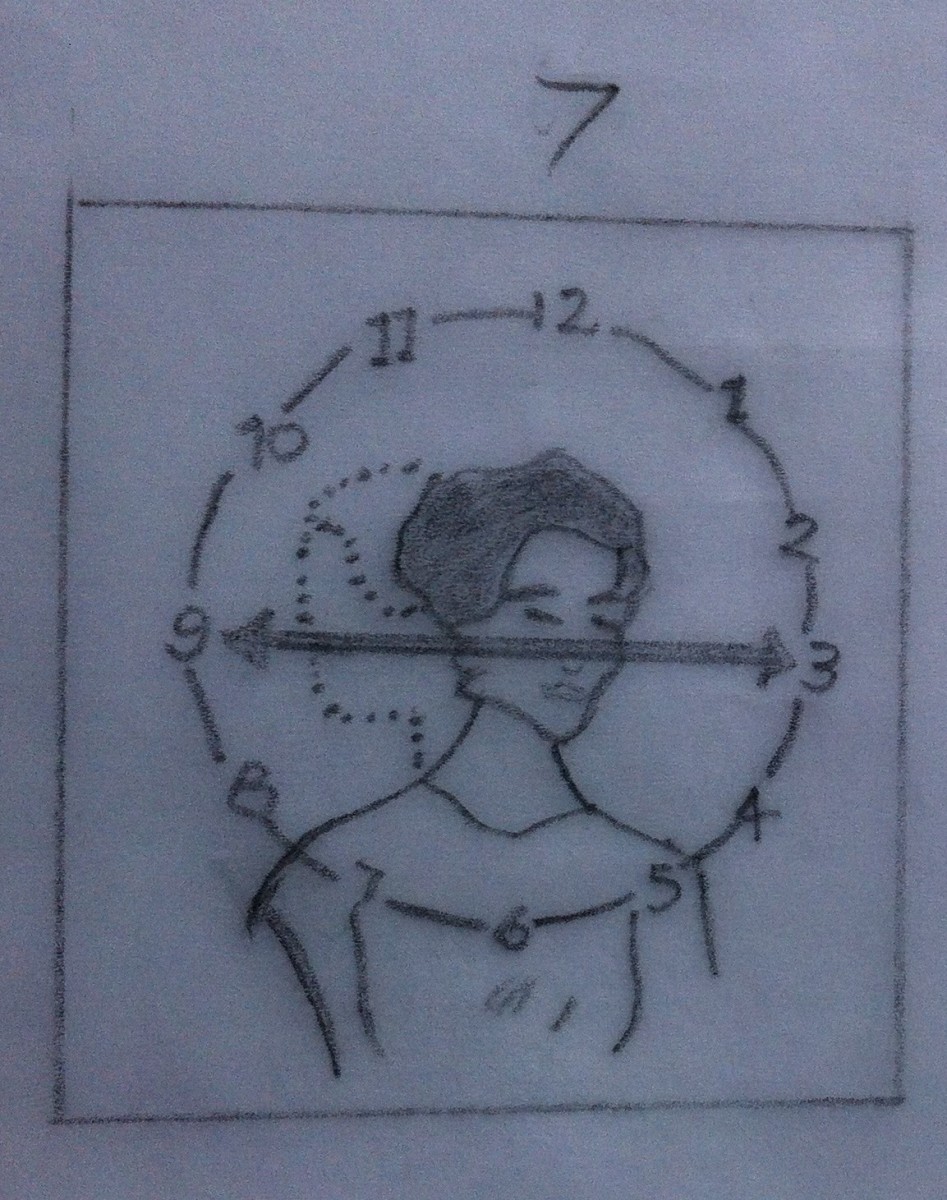
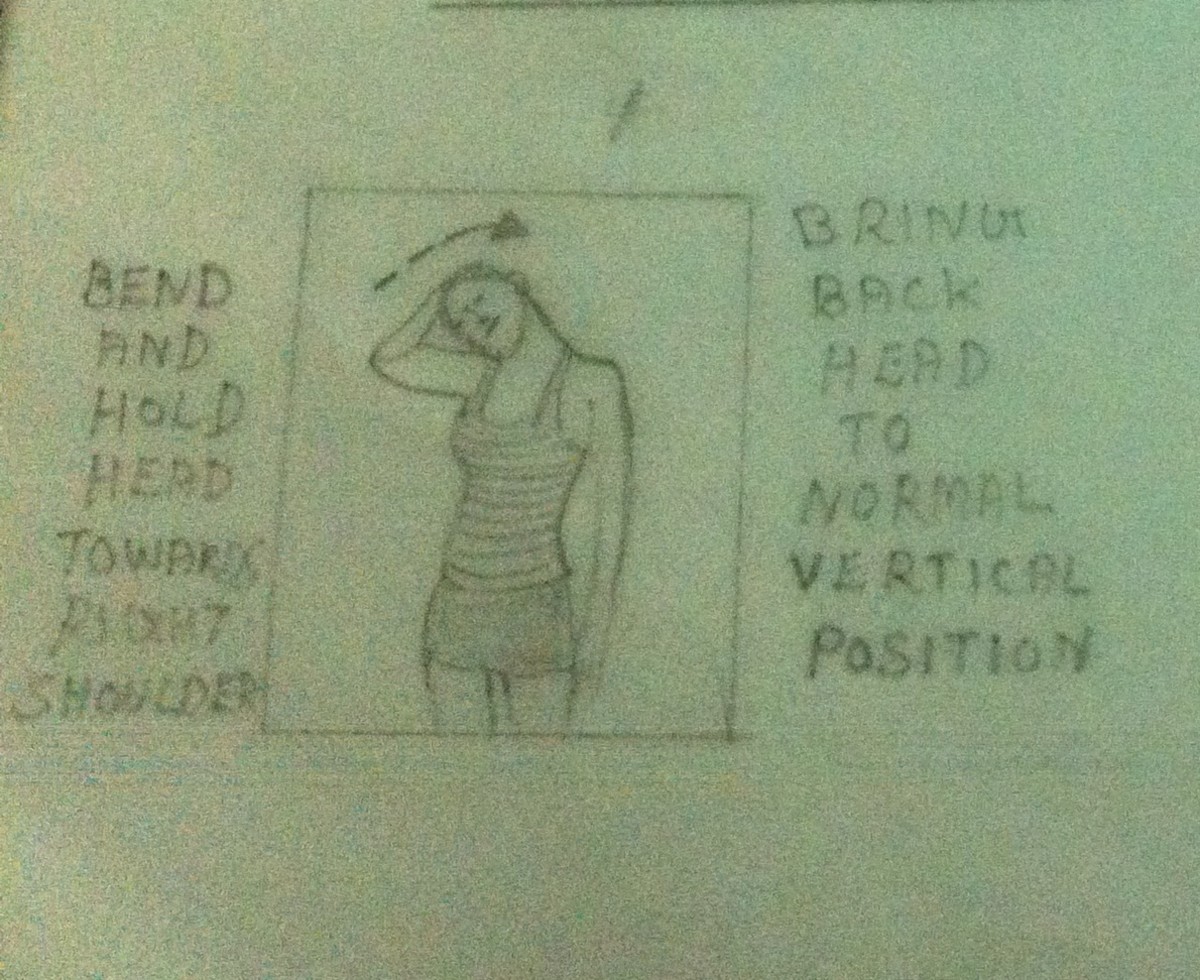
5. Mobilization Exercises – Mobilization Exercises to the cervical spine are indicated, once the acute stage has subsided. Active and carefully guided passive ranges of motion exercises to the cervical spine are advisable. Forceful manipulation exercises are to be avoided. Forceful manipulations will cause further damage and injury to the already compressed cervical cord and the nerve roots. Mobilization exercises which aggravate the symptoms must also be avoided. Exercises must be done within the limits of pain. Movements in the painful directions may be avoided. In short, one should be extra cautious in choosing the suitable mobilization exercises. To start with the exercises must be done in small ranges. Slowly and gently the ranges may be increased in a graded way. These exercises may be done 5-10 times (3-4 times a day). It is suggested that either ice or heat is applied prior to the commencement of the exercise program. Both in flexion and extension of the cervical spine there may be folding of ligamentumflavum. This folded ligamentumflavummay encroach upon the contents of the spinal canal and compresses the spinal cord. Hence flexion and extension of the spinal cord may aggravate the symptoms. Hence flexion and extension exercises to the cervical spine must be given with caution.
Please refer my earlier article ‘Mobilization Exercises to the Cervical Spine’ for more details.
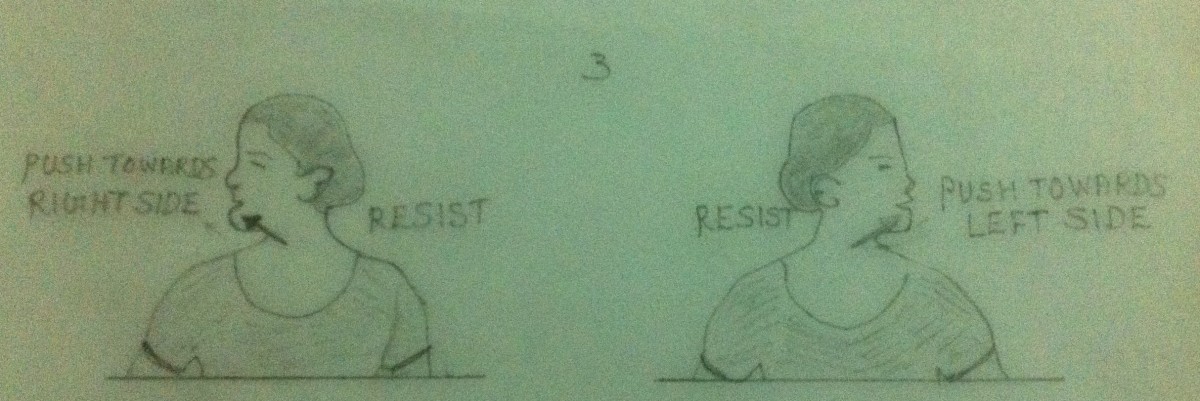
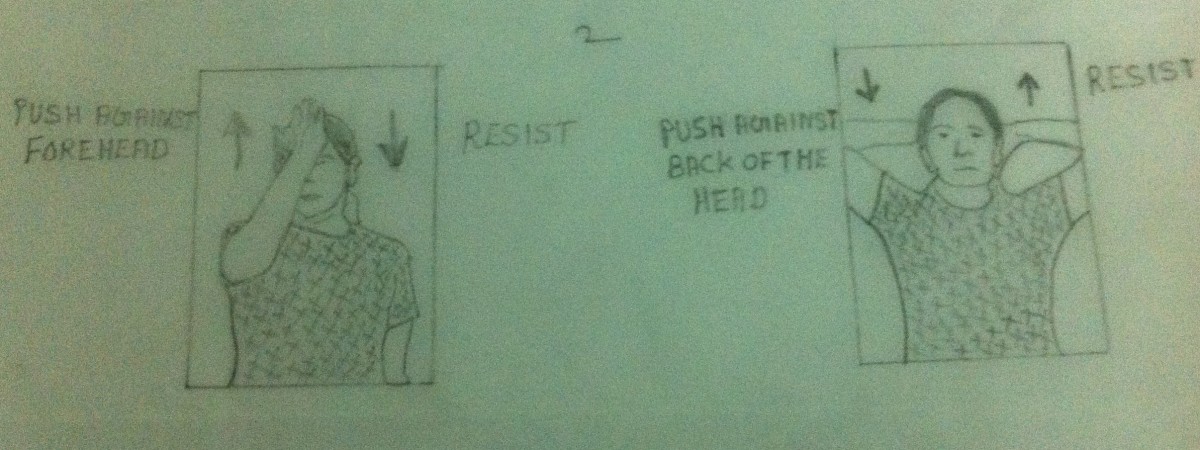
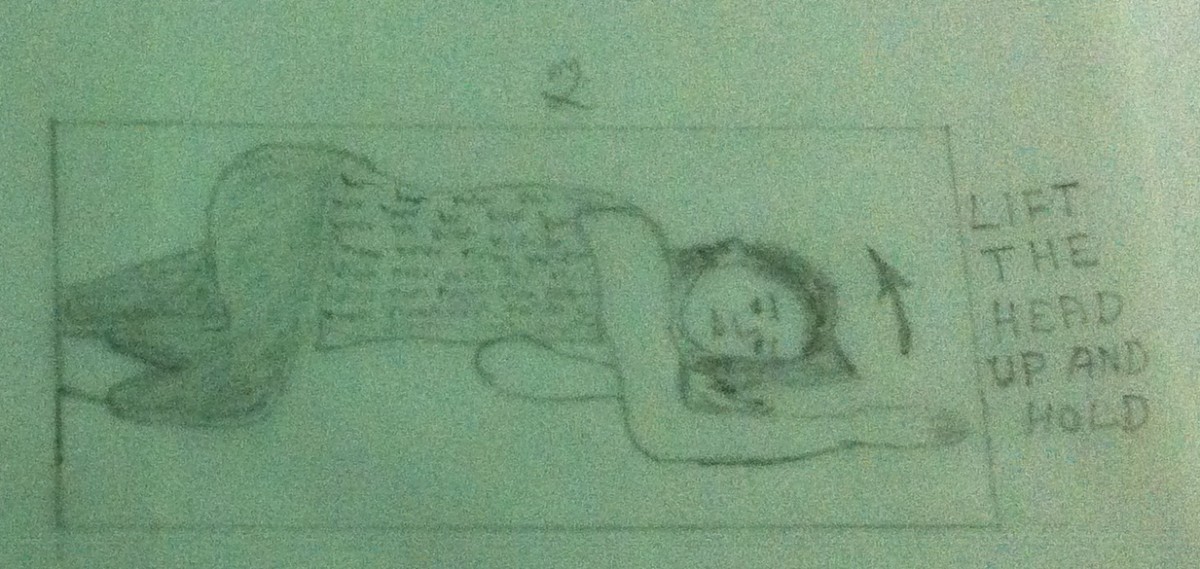
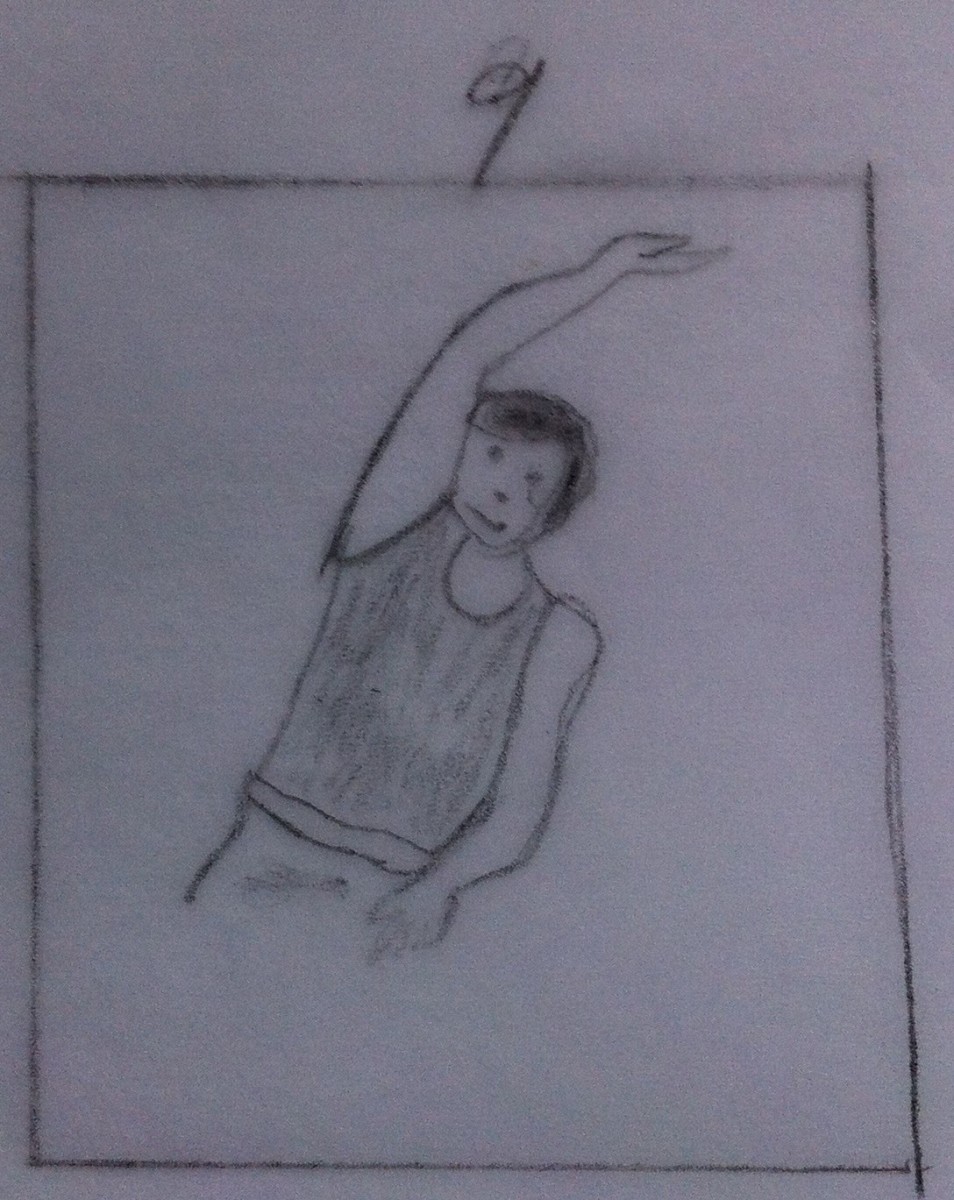
6. Strengthening Exercises – Mobilization exercise may be followed by strengthening exercise to the cervical spine. Usually mobilization and strengthening exercises may overlap. Ice or heat may be applied prior to the commencement of the exercise program. Avoid exercises that may aggravate the pain and the symptoms. Care should be taken in the appropriate selection of exercises. Do the exercises 5-10 times (3-4 times a day). To start with isometric exercises are preferred. Active and isotonic exercises may follow.
Please refer my earlier article ‘Strengthening Exercises to the Cervical Spine’ for more details.
Strengthening Exercises may also be given to the upper extremities and the lower extremities if there is weakness. The intrinsic muscles of the hand may be weak if there is nerve root compression in addition to the cord compression. In such cases strengthening exercises to the intrinsic muscles of the hand may be given.
Strengthening Exercises to the intrinsic muscles of the hand will be discussed later.
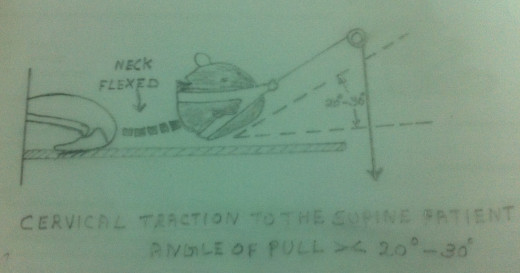
7. Cervical Traction – Cervical Traction may be given either manually or mechanically. Cervical Traction in the case of Cervical Spondylotic Myelopathy has not been proven to be of great value. But it helps in relieving symptoms due to nerve root compressions. Any way cervical traction in Cervical Spondylotic Myelopathy is not contraindicated. However, cervical traction must be discontinued forthwith if it aggravates the symptoms.
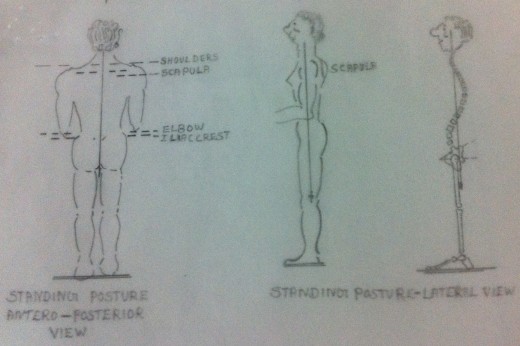
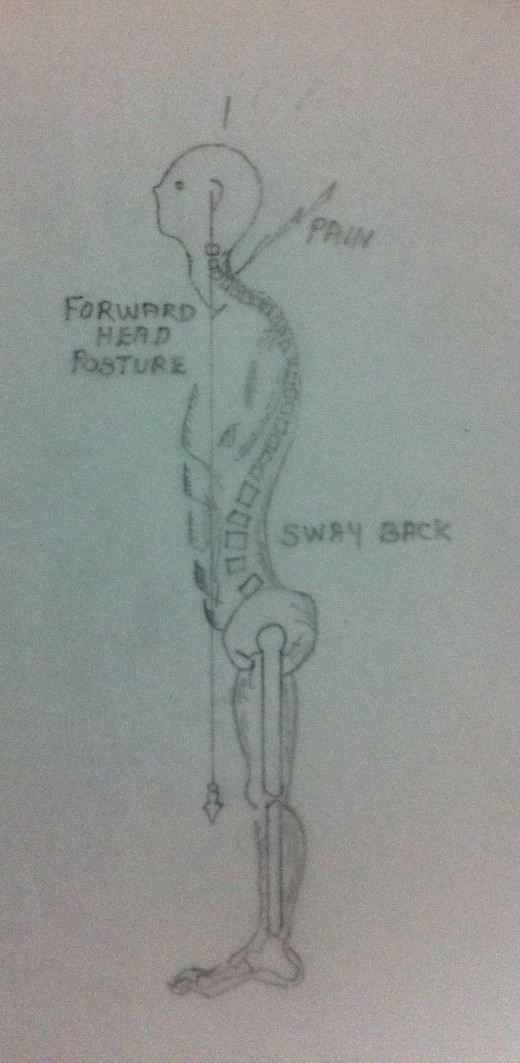
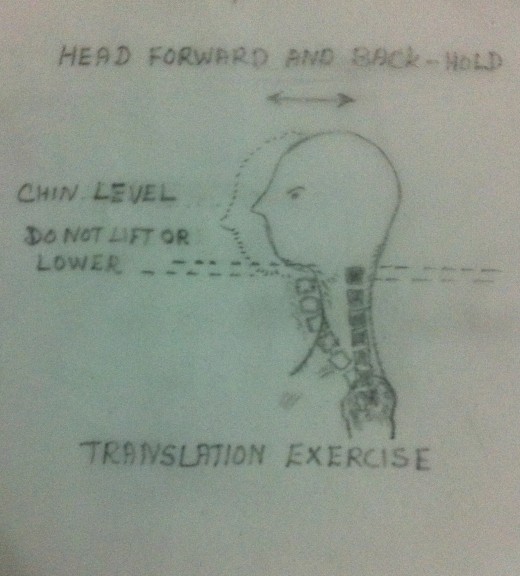
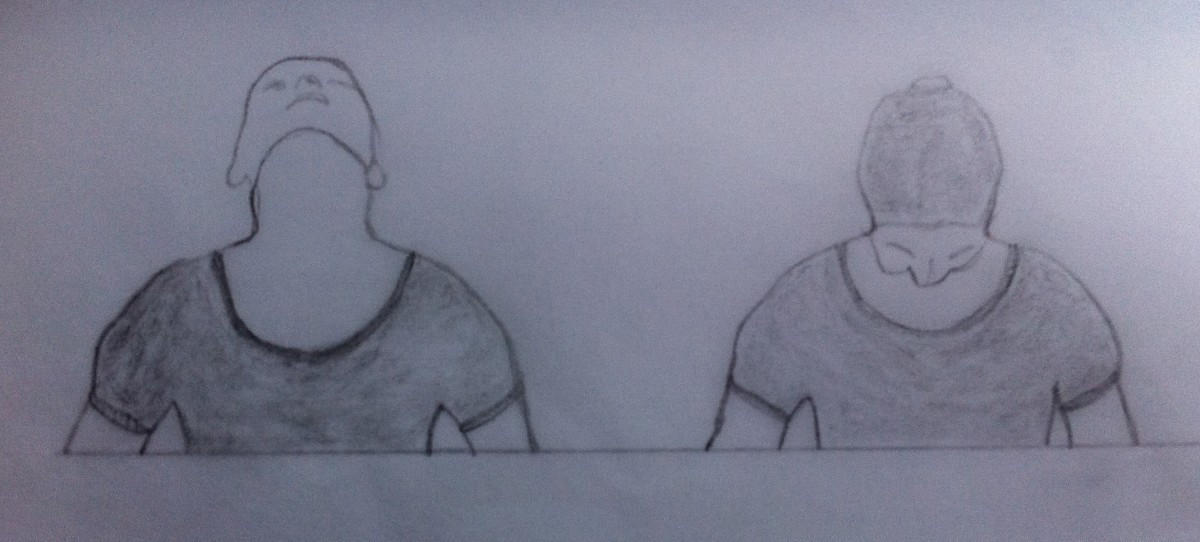
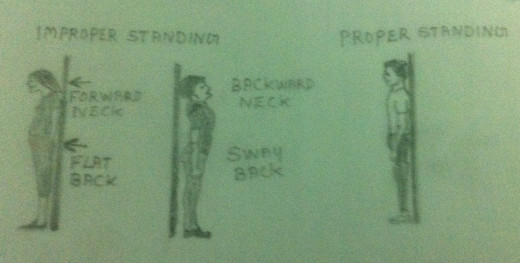
8. Postural Corrective Exercises – Faulty postures are considered as one of the most important causes leading to Cervical Spondylotic Myelopathy. This is because the faulty posture leads to trauma to the various structures of the musculoskeletal system surrounding the cervical spine and also the vertebral column itself. Even if proper treatment and exercises are provided the symptoms may not get relieved if there is faulty posture. Faulty posture aggravates the disease condition and the symptoms get worsened. Usually the faulty posture may be a ‘forward- head’ and ‘rounded upper back’ one. This posture causes excessive increased lordosis and excessive weight bearing on the neck.As a result there will be degenerative changes in the intervertebral discs and in the cartilages of the posterior facet joints. This leads to encroachment into the foramina causing nerve root compression and into the spinal canal causing cord compression. Postural corrective exercises must be taught to the patient. A conscious effort on the part of the patient is essential for correcting the faulty posture.
Please refer my earlier article on ‘Postural Corrective Exercises’ for more details.
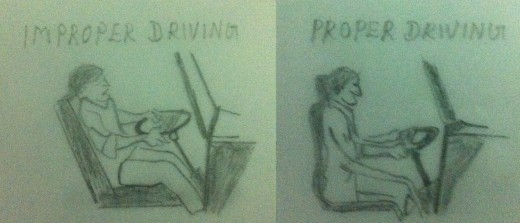
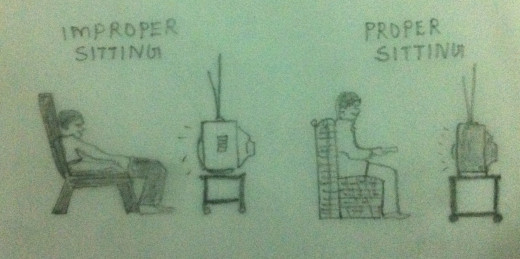
9. Activities of Daily Living – A thorough evaluation of the activities performed by the patient is very important. After evaluation, modifications must be made in the way of doing various activities so that any position that can aggravate the patient’s cervical condition or that aggravates the symptoms can be avoided. A conscious effort on the part of the patient is essential in carrying out the activities of daily living, maintaining a correct posture. Doing the activities of daily living in the correct proper way helps in preventing the worsening of the disease condition.
Please refer my earlier article ‘How to Take Care of Your Neck?’ for more details.
10. Co-ordination Exercise – Inco – ordination may be present in the involved limbs. Information regarding the whereabouts of the body in space, the position of the joints and the tension in the muscles forms an essential part of the data upon which the neuromuscular co-ordination is based. Lesion causing loss of any of this information will lead to in co - ordinated movement. The co – ordinated movement which is smooth, accurate and purposeful is brought about by the integrated action of many muscles and muscle groups. Substitution of the sense of sight to compensate for the loss of kinaesthetic sense forms the basis of re-education of co-ordinated movements. Dr.Frenkel tried to establish voluntary control of movement by the use of any part of sensory mechanism which remained intact, preferably sight, sound and touch, to compensate for the loss of kinaesthetic sensation.
Frenkel’s Exercises will be dealt with in detail in the next article.

11. Gait Training – The lower limbs are dedicated to the vital tasks of weight bearing and ambulation. The human gait pattern is defined as the way how the people walk. The normal gait contributes, to a great extent, in maintaining normal upright posture. Normal gait and good balance are essential in performing the normal activities of daily living without the fear of falling. Once the proper gait is maintained, one can carry out the activities of normal daily living with maximum mechanical advantage. Usually in the case of Cervical Spondylotic Myelopathy the patient has a wide based gait i.e. an abnormal gait. It is to be noted that in the case of a normal gait, the width of the base should not be more than 2-4 inches from heel to heel. In the case of Cervical Spondylotic Myelopathy the patient used to have a base wider than the normal gait. The patient usually walks with a wider base if they feel dizzy or unsteady due to cerebellar problems or due to cervical cord compression sequelae. Patients with sensory deficit in the sole of the feet will also have a wide based gait. Hence gait training is an integral part of the treatment prescribed for a patient suffering from Cervical Spondylotic Myelopathy.
Gait Training Exercises will be dealt with in detail in the next article.






