Clinical Relevance Of Rheumatoid Arthritis: Diagnosis, Differential Diagnosis And Prognosis

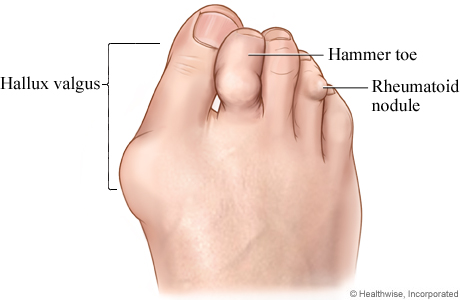
Hammar Toe And Rheumatoid Nodule
Diagnosis
The diagnosis is to be made on clinical examination and laboratory criteria. Since clinically, several conditions resemble rheumatoid arthritis, diagnostic criteria have been laid down. The diagnostic criteria for rheumatoid arthritis (As set forward by the American Rheumatism Association) are as follows:
- Morning stiffness of more than 30 minutes duration.
- Pain or tenderness in at least one joint
- Swelling of at least on joint as observed by a physician
- Swelling of at least one other joint as observed by a physician, with a three month interval between the appearance of the 2 joint swellings.
- Symmetrical swelling of identical joints except distal interphalangeal joints.
- Subcutaneous nodules.
- X-ray changes of RA
- Positive Rose- Waaler test
- Poor mucin clot in synovial fluid
- Histology of synovial membrane showing at least 3 of the following features: (a) vilous hypertrophy, (b) lymph follicle formation, (c) superficial synoviocyte hyperplasia, (d) fibrinoid necrosis and (e) foci of cell necrosis.
- Characteristic biopsy evidence in the nodules. (Note: Criteria 1-4 should be present for at least six weeks).
If 7/11 criteria are present, it is called classical rheumatoid arthritis, 5/11 is called definite rheumatoid arthritis and 3/11 probable rheumatoid arthritis, provided the duration of the disease is at least four weeks. The term ‘possible rheumatoid arthritis’ denotes the presence of any of the following.
- Morning stiffness
- Pain and tenderness of joint
- History of joint swelling observed by physician
- Subcutaneous nodules
- High ESR
For at least 6 weeks duration.
Inflammed Fingers

Rheumatoid Diseases

Differential Diagnosis And Prognosis
Differential Diagnosis
Rheumatoid arthritis has to be distinguished from rheumatic arthritis in which children are more affected, the joint lesions are migratory, large joints are affected, effusion is prominent and ASO titer is high. In psoriatic arthritis, there is invariably evidence of psoriasis of the skin or nails and the arthritis involves the small joints of the hands (especially distal interphalangeal joints) and feet more. The hand may be severely mutilated (arthritis mutilans). Involvement of the sacroiliac joints and spine is not uncommon.
Several joints may be affected in gout. The metatarsophalangeal joint of the big toe is characteristically affected more frequently, though any joint may be involved. In chronic tophaceous gout, tophi may be seen as nodules around the joints, especially the elbow. Osteoarthritis affects elderly subjects. Common joints affected are the spine, hips, knees and distal interphalangeal joints. Heberden’s nodes may be seen at the base of the distal phalanges. The condition is progressive. The ESR is generally normal or only moderately elevated.
Allergic arthritis manifests as arthralgia and arthritis involving several joints, both proximal and distal. Permanent deformity does not occur. Other manifestations of allergy may be evident. The ESR is only moderately elevated and not to the high levels seen in rheumatoid disease.
Other conditions which may mimic rheumatoid arthritis are syphilitic arthritis, gonococcal arthritis, Reiter’s syndrome and ankylosing spondylitis. In ankylosing spondylitis, the sacroiliac joints and spine are maximally affected. Peripheral joint involvement is less common.
Prognosis
In general, the disease tends to become recurrent and chronic and in may cases, it leads to considerable disability and deformity. Favourable criteria are: acute onset, male sex, onset of late age, asymmetrical or mono-articular involvement, negative rheumatoid factor, absence of subcutaneous nodules, absence of vasculitis and prompt response to therapy early in the disease.
© 2014 Funom Theophilus Makama
Related

Rheumatism and Arthritis - Symptoms, Causes and Its Control With Natural Home Remedies

Rheumatoid Arthritis Management: Comprehensive Overview

Conventional Rheumatoid Arthritis Treatments

Kidney Pain: Location, Diagnosis and Treatment

Encephalomalacia - Symptoms, Prognosis, Treatment, Causes, Diagnosis



