Coxsackie Virus Infections: Health Implications, Pathogenesis, Clinical Manifestations, Diagnosis And Treatment

Physical Presentation Of The Coxsackie Viral Infection
Health Implications Of Coxsackie Viral Infection
Coxsackie viruses are picorna viruses which can be grouped into A and B. They were first isolated from the village of Coxsakie in New York by Dalldorf in 1948, hence the name is derived from there. About 30 immunological types have been isolated. Many strains are commensals in the alimentary and respiratory tract of man. Spread is by the fecal-oral route and small outbreaks occur especially in summer. The causative role of these viruses in any specific illness can be established only by isolating it from specific lesions in the affected organs, or tissue fluids.
Pathogenecity: Several lesions are produced by these viruses group A and B. These include
- Neurological lesions
- Respiratory disorders
- Carditis
- Hand-foot mouth disease and others.
The incubation period is 2 to 14 days. Neurological lesions include polio-like paralysis, meningoencephalitis and aseptic meningitis. Neuronophagia of the anterior horn cells in the spinal cord and perivascular infiltration by lymphocytes are the histological features. In fata group B infections, meningoencephalitis and scattered foci of degeneration in the cerebral hemisphere, pons, cerebellum and spinal cord are seen, the spinal cord is extensively involved.
Devil’s Grip Bornholm’s Disease In Coxsackie Viral Infection

Clinical Manifestations Of Coxsackie Viral Infection
Respiratory lesions: Pleura is most characteristically involved. The syndrome of pleurodynia (devil’s grip Bornholm’s disease, epidemic myalgia) is caused by Coxsackie B group viruses.
Severe pain develops in the chest and upper abdomen, after a prodromal febrile illness. Breathing becomes painful, short, shallow and rapid. Physical examination may reveal pleural rub, pleural effusion, pneumonia, myocarditis, pericarditis, hepatitis or orchitis. The cute phase subsides in 2 to 3 days but mild fever and pain may persist for a longer period. Pleurodynia has to be distinguished from acute myocardial infarction, other forms of pleurisy and surgical abdominal emergencies. Symptomatic treatment with rest and analgesics gives relief.
Cardiovascular lesions: The heart is affected by both groups of Coxsackie viruses, but group B is more common to produce acute myocarditis and pericarditis. Infection acquired congenitally or neonatally tends to be serious and rapidly fatal. This may be associated with encephalitis, hepatitis or adrenal necrosis. Pericarditis is more common in older children and adults. Myocarditis may lead to cardiac failure, arrhythmias or the later development of chronic cardiomyopathy and calcific or constrictive pericarditis. Electrocardiographic changes may occur. Congenital heart disease is associated with Coxsackie B types 3 and 4 infection acquired in utero.
Other manifestations: Coxsackie viruses have been implicated in the production of herpengina (painful vesicles in the throat and pharynx), lymphonodular pharyngitis, hepatitis, exanthematous fevers and pancreatitis.
Laboratory diagnosis: It is aimed at isolation of the virus and demonstration of rising titers of antibodies.
Treatment: There is no specific therapy. Majority of the cases recover completely in one to seix weeks. Absolute bed rest and symptomatic treatment should be continued till the ECG becomes normal.
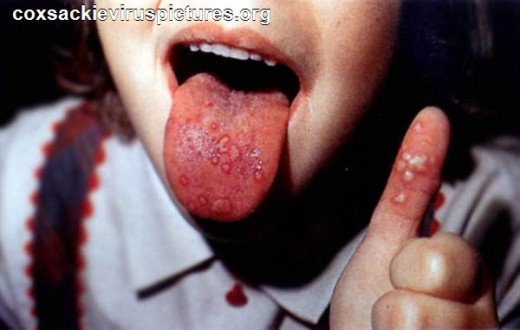
The Physical Presentations Of Hand-Foot And Mouth Disease

Infectious Diseases

Hand-Foot And Mouth Disease
Infections caused by Coxsackie viruses types A4, 5, 7, 9, 10 and 16 give rise to a febrile illness followed by superficial vesicular eruptions inside the mouth, fingers, palms and soles. Occasionally, small outbreaks may occur. The whole course lasts for 4 to 8 days after which the vesicles develop into shallow ulcers which heal completely without leaving behind any scar.
Diagnosis: Hand-foot and mouth disease may be mistake for chickenpox, aphthous stomatitis or herpangina. In chickenpox, the vesicles are more widely distributed, multiple crops occur and postulation and scab formation are seen. These are absent in hand-foot and mouth disease. The virus can be isolated from the vesicle fluid. Neutralizing and complement fixing antibodies are also demonstrable. Treatment is essentially symptomatic.
© 2014 Funom Theophilus Makama
Related

Zika Virus Disease, Microcephaly, and Guillain-Barré Syndrome

Staph Infection: Causes, Contagious, Symptoms, Treatment, and Pictures

Clinical Manifestations Of Hypothyroidism: Cretinism, Myxedema, Hoffman’s Syndrome And Pendred’s Syndrome
"Star Trek" Episodes About Viruses, Epidemics, and Pandemics

Measles and Rubella Facts, Similarities, and Differences


