Frozen Shoulder - Physiotherapy Treatment #1

Introduction
Frozen Shoulder, otherwise known as Adhesive Capsulitis, is a condition which is characterised by stiffness, pain and limitation of range of motion of the shoulder. The term Frozen Shoulder is sometimes incorrectly used for Arthritis. But it is to be noted that both are not related. Frozen Shoulder relates to shoulder joint only whereas Arthritis relates to multiple joints. Adhesive Capsulitis is derived from Latin words ‘adhaerens’ meaning ‘sticking to’ and ‘capsula’ meaning ‘little container’ and the Greek word ‘itis’ meaning ‘inflammation’
How Shoulder Joint works?
Shoulder Joint is a multi-axial ball- and- socket type of synovial joint. It possesses three degrees of freedom of movement. Shoulder Joint, in the strict sense, is also called the Glenohumeral Joint. In the Glenohumeral Joint the ‘ball’ is represented by the spheroidal ‘head of humerus’ (the bone of the upper arm), which forms about one- third of a sphere. The ‘socket’ is formed by the pear shaped small and shallow cavity called the ‘glenoid cavity’ of the scapula, the shoulder blade. The ‘head of the humerus’ is much larger in extent than the ‘glenoid cavity’. The ‘ball’ of the proximal end of humerus (ie. the head of humerus) articulates with the ‘glenoid cavity’ of the scapula. The ligaments, the muscles and the tendons support the Glenohumeral Joint. The bony parts which constitute the Glenohumeral Joint and the ligaments and the tendons that support the joint are encased in a Capsule called the ‘Joint Capsule’. Joint Capsule is formed of connective tissue and it is loosely attached. Hence it permits free movements of the Glenohumeral Joint.
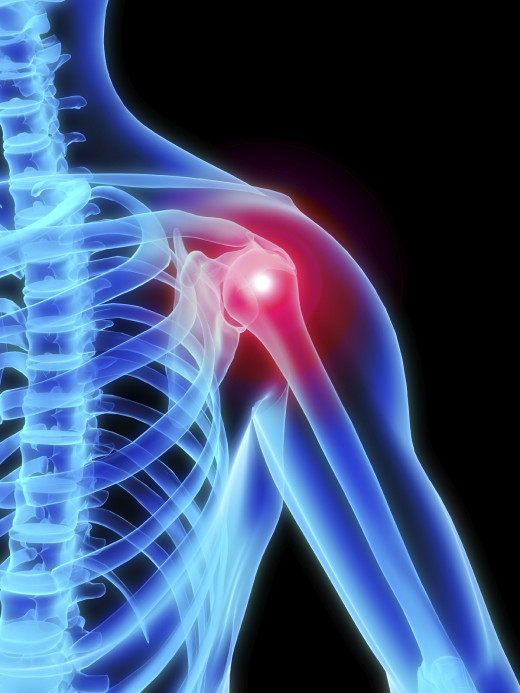
What Happens in Frozen Shoulder?
The Joint Capsule which is loosely attached around the shoulder joint (Glenohumeral Joint), becomes inflamed. This inflamed Joint Capsule, in a period of time, swells and thickens and gets transformed into thick bands of scar tissue. These thick bands of scar tissue gets adhered around the shoulder joint (Glenohumeral Joint) and tightens the joint. Moreover adhesions may be formed on the inner side of the Joint Capsule. As a result of adhered Joint Capsule and the adhesions there is less room for the head of humerus to articulate with the ‘glenoid cavity’ of the scapula. Moreover there may be deficiency of synovial fluid. Hence there will also be lack of lubrication in the joint. All these factors contribute to the stiffness of the joint, pain and the limitation of movement of the shoulder joint (Glenohumeral Joint).
Three Stages of Frozen Shoulder
Signs and Symptoms evolve gradually, worsen over time and finally resolve within one or two years. The normal course of Frozen Shoulder is described as having three stages.
Stage 1- The first stage is the ‘freezing stage’ or the ‘painful stage’. This stage usually lasts for 6 weeks to 9 months. During this stage pain is felt with any movement of the shoulder. Moreover there will be stiffness and limitation of movement of the shoulder.
Stage 2- The second stage is the ‘frozen stage’ or the ‘adhesive stage’. This stage usually lasts for 4 months to 9 months. During this stage there is slight improvement of pain whereas the stiffness of the shoulder remains the same or may get worsened. It is to be noted that the range of motion of the shoulder joint may be decreased notably.
Stage 3- The third stage is the ‘thawing stage’ or the ‘recovering stage’. This stage usually lasts for 5 months to 26 months. During this stage there may be relief of pain. But there may be recurrence of pain. There may be improvement of range of motion also. But there will not be full recovery of range of motion. There will be a residue. But by the passage of time, even though the range of motion is not attained fully, the patient might get adjusted with the disability. He may carry out the activities in his own way and may have a feeling of relief. But it is always advisable to undergo physiotherapy treatment till the full recovery is attained and the residue is a minimum.
Causes
Causes are not fully understood in some cases ie. the causes are unidentifiable. The usual causes can be summarized as follows –
- Prolonged immobilization of shoulder in case of fractures in the upper limb bones.
- Rotator Cuff Muscles injury. Supraspinatus Tendinitis with or without partial rupture of the tendon.
- Hemiplegic Patients.
- Any trauma to the shoulder including contusion.
- Prolonged immobilization of shoulder following surgeries in the upper limbs.
- Diabetes – 2 to 4 times likely to get Frozen Shoulder, but the reason is unknown. The Diabetic patents are likely to get Frozen Shoulder bilaterally. If the sugar level is brought under control there may be relief of pain to certain extent. Frozen Shoulder is more troublesome in Diabetic patients. In such patients long period of treatment is required to achieve relief.
- Cervical Spondylosis- more prone to get Frozen Shoulder, but the reason is unknown. The Cervical Spondylosis patients are likely to get Frozen Shoulder bilaterally.
- Patients with Cardiovascular Diseases- less common.
- Patients with Lung Diseases-less common.
- Hyperthyroidism and Hypothyroidism.
- Parkinson’s disease.
- Mastectomy- surgical removal of breast.
- Rheumatic Diseases.
- Tuberculosis.
Incidence
Age- Most often between 40 and 70 years. Rarely below 40 years.
Sex- More often in women. 70% of people with Frozen Shoulder are women.
Side- Unilateral or Bilateral.
Signs and Symptoms
- Pain in the shoulder – Pain usually constant. Worse at night and with cold weather. Disturbed sleep due to pain. Pain will be worse if lying still. Unexpected movements or jerks can provoke episodes of tremendous pain or aching. Sometimes leads to cramping.
- Tenderness – Usually the anterior capsule of shoulder joint is tender.
- Radiating Pain – Rarely pain may radiate down the arm along the course of certain nerves.
- Stiffness – The patient feels stiffness of the shoulder joint. There is limitation of range of motion of the shoulder in all directions. Especially the external rotation of the shoulder joint is restricted.
- Stiffness of neck – The movement of Cervical Spine may be limited.
- Weakness – There may be weakness of muscles around the shoulder joint.
- Disuse Atrophy – There may be atrophy of muscles around the shoulder joint due to disuse.
- Psychological problems – Depression and lack of concentration.
- Pain and swelling of joints of hand – Frozen Shoulder may lead to Shoulder Hand Syndrome at a later stage. In such cases there may be swelling and pain of the small joints of the hand.
- Masking of Shoulder Joint Movements – Shoulder movements (Glenohumeral joint movements) are usually masked by Scapulothoracic Gliding Movement. The patient may misunderstand the Scapulothoracic Gliding Movement for the Shoulder Joint Movement.
Investigations
- Physical Examination
- X-ray
- Ultra Sound Scan
- MRI Scan
- Other Routine Examinations to rule out other conditions.
Prevention
- Early consultation with a doctor and a physiotherapist during the early stage of shoulder pain.
- Start physiotherapy treatment at the early stage itself.
- Home Program as directed by the physiotherapist.
- Stabilize the other primary disease conditions such as Diabetes.
Treatment
- Non Steroid Anti- inflammatory Drugs.
- Pain Relievers.
- Corticosteroids- Resort to Corticosteroids only if physiotherapy fails.
- Steroid injections – Injecting Corticosteroids into the joint may help to decrease pain and improve shoulder joint mobility. Resort to Steroid injections only if physiotherapy fails.
- Joint Distention – Injecting sterile water into the joint capsule can stretch the joint capsule and make the joint easier to move- only if physiotherapy fails.
- Arthroscopic Surgery – Arthroscopically, the scar tissue and the adhesions within the joint capsule may be removed. Need physiotherapy after the procedure.
- Shoulder Manipulation under Anaesthesia – The surgeons manipulate the shoulder joint under anaesthesia and move the joint in all directions. Under the influence of anaesthesia the patient does not feel any pain while doing manipulation. This type of manipulation may loosen the tight and adhered joint capsule to some extent. This procedure has to be carried out very carefully and judiciously as it may lead to further damage to the joint. This is because the patient won’t be in a position to respond, since he is under the influence of anaesthesia, even if the intensity of the manipulative techniques applied goes beyond the permissible limits and excessive force is applied. It is also to be noted that even after the manipulation of shoulder joint is done under anaesthesia, the shoulder joint presents with residual stiffness and pain. The degree of residual stiffness and pain varies from patient to patient and it still interferes with the quality of life of the patient. Hence he may have to undergo physiotherapy treatment even after shoulder manipulation under anaesthesia. Hence it is advisable that one may resort to Shoulder Manipulation under Anaesthesia only when physiotherapeutic manipulation fails.
- Occupational Therapy.
- Physiotherapy – will deal with separately. Always consult an experienced ‘hands- on physiotherapist’ who is well proficient is ‘physiotherapeutic manipulative techniques’.
- Home Program – Has to carry out exercises to the shoulder joint as home program. A regime of exercise program may be prepared in consultation with the physiotherapist.





