Gait Training – Swing Phase – An Analysis – Variations in Normal Gait

Introduction
As we have already discussed, the normal walking cycle has two phases.
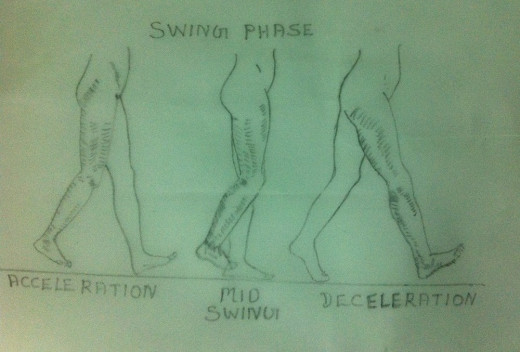
They are Stance Phase i.e. when the foot is flat on the ground and the Swing Phase i.e. when the foot is off the ground and moving forward. 60% of the normal walking cycle is spent on Stance Phase and the remaining 40% is spent on Swing Phase. The Swing Phase has three smaller components. They are Acceleration, Mid Swing and Deceleration.
Most of the problems of the gait become apparent and evident when the patient is on the Stance Phase. This is because the Stance Phase is the weight bearing part of the walking cycle. More over 60% of the walking cycle is spent on the Stance Phase. Because of these two reasons, the lower limb is subjected to greater and continuous stress and strain resulting in variations in gait. Only fewer problems become apparent and evident in the Swing Phase because this phase is not a weight bearing phase. More over the patient spends only 40% of the walking cycle during the Swing Phase. Hence the stress and strain in the lower limbs is very minimal during the Swing Phase.
Now let us examine and analyse the Swing Phase and try to find out how various problems of the lower limbs interfere with each joint during different components of Swing Phase.

1st Component–Acceleration
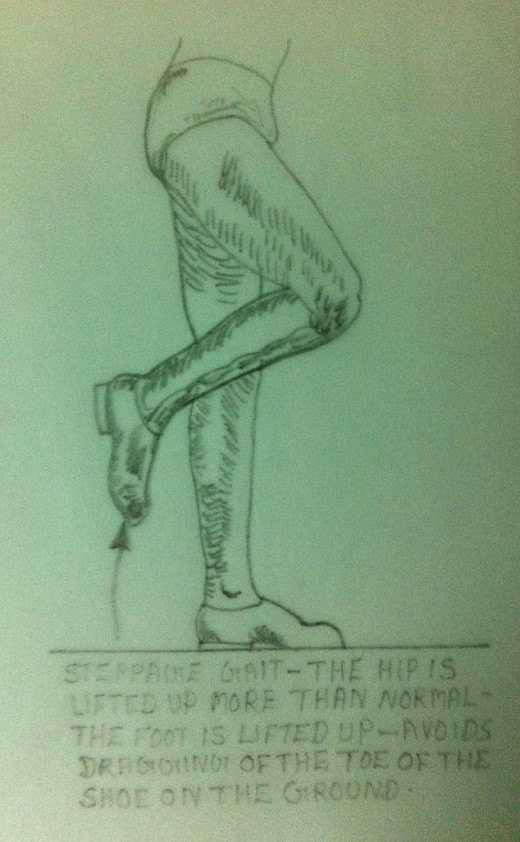
Foot – During the entire Swing Phase, the dorsiflexors of the ankle are active. During Swing Phase the dorsiflexors of the ankle contract and hold the foot up shortening the lower limb. This enables the patient to bring the foot forward without any hindrance or dragging on the ground. The patients with weak dorsiflexors of the foot have a ‘foot drop’. In such a case there is every possibility that the foot drags on the ground in the case of Swing Phase. To avoid this ‘dragging of the foot on the ground’ the patient with a ‘foot drop’ flexes the hip more than normal so that the knee and the foot are lifted up further, thus avoiding ‘dragging of the foot on the ground’ during Swing Phase. Such a gait is called ‘High-Step Gait’, or ‘Steppage Gait’, or ‘Foot-Drop Gait’.
Knee-During the Swing Phase the hip and the knee are flexed. The knee flexion is the maximum between Toe–0ff and Mid Swing. This shortens lower limb and hence the limb can move forward without touching the ground.
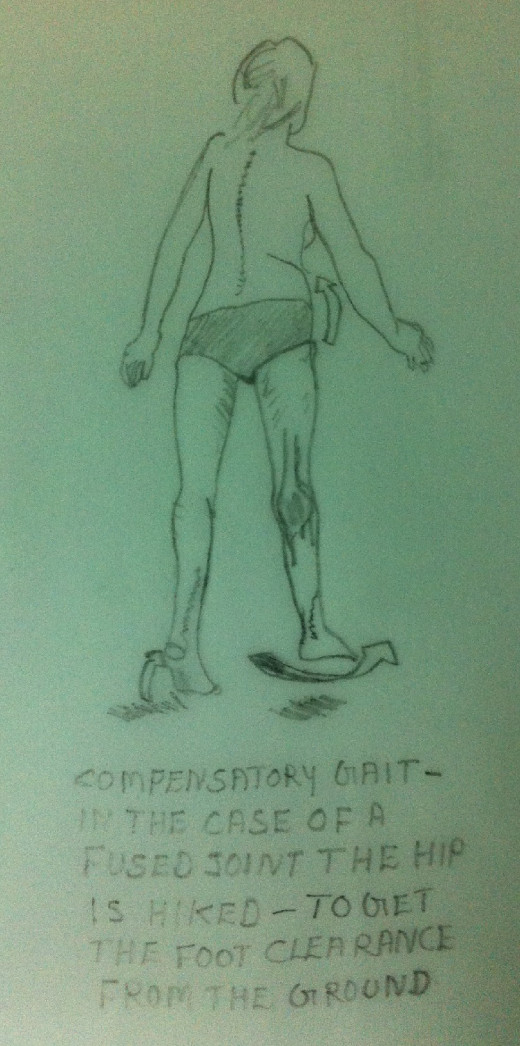
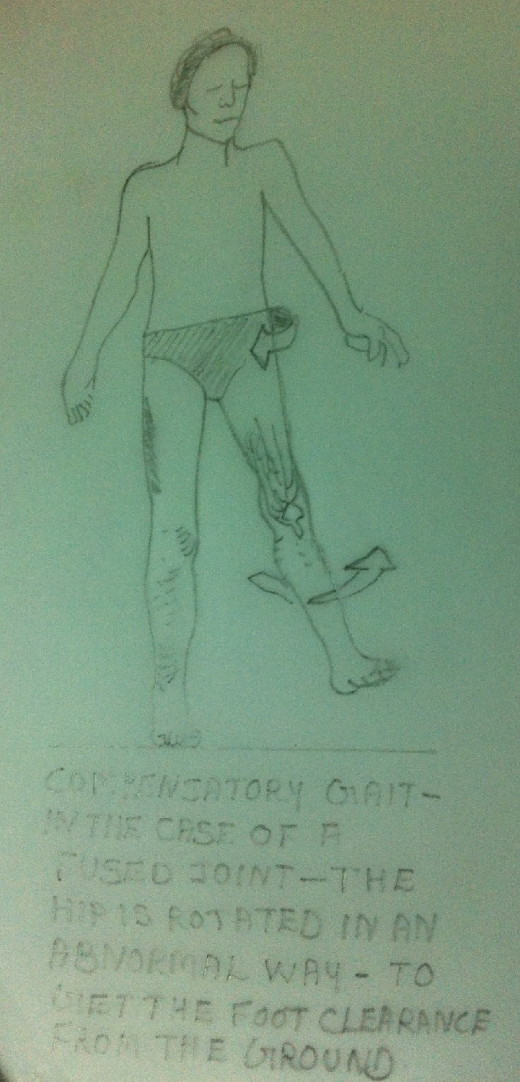
Hip-The Quadriceps Muscle begins to contract just before Toe-off to help to initiate the forward swing of the leg. In the case of a patient with weak Quadriceps this initiation does not happen. In such cases, the patient may rotate the pelvis anteriorly in an exaggerated manner to provide a forward swing to the limb. In cases where there is fusion of hip or knee, the patient hikes the hip so that the foot can clear the ground during Swing Phase.
2nd Component – Mid Swing
When the dorsiflexors are weak, the patient will have a foot drop. Hence in the Mid Swing, he may drag the foot on the ground. To avoid this, the patient may flex the hip more than normal so that the knee and the foot are lifted up further thus avoiding ‘dragging of the foot on the ground’. This gait is called ‘High Step Gait’, or ‘Steppage Gait’, or ‘Foot Drop Gait’.
3rd Component – Deceleration
Just prior to the heel strike, the Hamstring Muscles contract to slow down swing so that the heel can strike the ground quietly and in a controlled manner. The patient with Hamstring Muscle weakness may not be able to decelerate properly and quietly before heel strike in a controlled manner. In such cases the heel strike may be harsh. This results in thickening of the heel pad. In such cases there may be hyper extension of the knee joint. Such a gait is called ‘Back Knee Gait’.


