Myositis Ossificans - Elbow Joint - Physiotherapy Treatment - 2


Treatment is primarily conservative as some patient’s calcification will spontaneously be reabsorbed and hence may have minimal symptoms.
A. Prevention
- Vigorous massage or vigorous passive stretching of the elbow joint must be avoided at any cost. Local bone setters or well -wishers of the patient must be dissuaded from handling elbow injuries. In all cases of elbow injuries, care must be taken that no massage or passive stretching is given to the elbow joint immediately after the removal of plaster.
- In all cases of elbow injuries, no treatment is attempted till a proper diagnosis is reached. Before resorting to treatment a thorough examination of the elbow joint is essential. X ray is very helpful.
- Even in the case of crack fractures of the lower end of humerus or neck of radius or in the case of severe contusions, it is advisable to rest the elbow joint for at least a minimum period of 3 weeks by providing a plaster slab.
B. Rest – Immobilization
- In suspected cases, the upper limb is rested and the elbow is put in flexion and supination. It is maintained by a sling. No movement is given to the elbow joint or to the radio-ulnar joint for 14-21 days.
- When a fussy ‘cotton wool appearance mass’ is noticed in the X-ray, the elbow is immobilized in flexion and supination with a plaster for 4 weeks. When the plaster is removed it is usually found that the movement of the elbow is improved. It is also found in the X –ray that the shadow like appearance is smaller but it becomes denser. Immobilization is continued further till there is maximum recovery of movement and the X- ray shows a well-defined homogenous calcified mass.
C. Cryotherapy – Application of Ice
In suspected cases of ‘Myositis Ossificans’ ice may be applied. Cryotherapy is highly beneficial in the acute stage. Crushed ice cubes wrapped in a thick towel is wrapped around the injured elbow for 20 minutes. Remove the ice for 10 minutes. Again apply the ice for 20 minutes. Repeat the whole procedure three times a day. Avoid direct application of ice as it may lead to ice burns. Cryotherapy helps in the following ways.
- It has analgesic effect and hence relieves the pain.
- It relieves muscular spasm and hence relieves pain.
- Once the pain is relieved, the range of motion of the joint may be increased.
- It stops the internal bleeding, if present.
- It causes alternate vasoconstriction and vasodilatation and thus encourages the healing process. It also enhances the deep arterial blood circulation.
D. Heat Application
Superficial heating modalities like Hot Water Fomentation, Infrared Radiation and Wax Bath are found to be very useful to relieve the pain and the muscular spasm in the chronic cases. Ultra Sound Therapy is also found to be useful in treating ‘Myositis Ossificans’. Hence the range of movement of the joint is also increased. Avoid heat application in the acute stage. The heat application will have almost all the effects as in the case of cold application.


F. Active Movements
Once the sling or the plaster is removed active movements may be encouraged. Heat or Cold may be applied prior to the exercise program. No attempt must be made by the physiotherapist or the patient himself to massage or stretch the elbow forcibly.
In the suspected cases of Myositis Ossificans, the elbow is rested in flexion and supination and is maintained in a sling for 14-21 days. When a ‘fussy cotton wool appearance mass’ is noticed in the X- ray, the elbow is immobilized in flexion and supination with plaster for 4 weeks. When the plaster is removed it is usually found that the movement of the elbow is improved. It is also usually found in the X-ray that the shadow like appearance becomes smaller but it becomes thicker and denser. Immobilization is continued further till there is maximum reabsorption of the bony mass so that the X-ray shows a well-defined homogenous calcified bony mass. Anyway, in most of the cases, there may be a residue of calcified bony mass present in the joint even after the stipulated periods of immobilization. This residual bony mass restricts the movement of the elbow joint and the radio-ulnar joints. This residual bony mass may impinge upon the soft tissues around the joint, thus causing discomfort and pain. The restriction of movements of the joints may also be due to the contractures of the muscles and the tendons around the elbow joint. The contracture of the joint capsule also contributes to the limitation of the movements of the joints .The degree of restriction of movement of the elbow joint depends upon the size of the residual bony mass. Moreover there may be weakness of muscles of the forearm. Once the sling or plaster is removed, active exercises may be encouraged. These exercises aim at improving the range of motion of the elbow joint and the radio- ulnar joints of the forearm. They also aim at strengthening the weak muscles and stretching of the contracted muscles of the forearm. Ie. The muscles around the elbow joint.
For Active Exercises please refer my earlier articles on ‘Tennis Elbow’. Most of the Active Exercises which I have dealt with in my earlier articles on ‘Tennis Elbow’ are suitable for ‘Myositis Ossificans’ also. Anyway it is advisable to seek the advice of a qualified physiotherapist who may help you to chart out a most suitable exercise regime for you. Following are two specialized mobilization techniques which are very much beneficial in treating ‘Myositis Ossificans.’

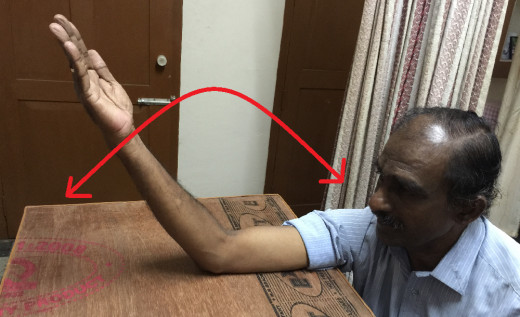
G. Hold Relax Exercise - 1
Let the patient has ‘Myositis Ossificans’ in his right elbow. Let there be limitation of extension of right elbow.
Starting position-The patient sits on a chair near a table facing it. The patient keeps his bend right elbow on the table in such a way that the elbow is bend approximately 45 degrees with the anterior aspect (front side) of the right forearm and the palmar aspect (front side) of the right hand is facing upwards with the right wrist and right fingers held extended (straightened).
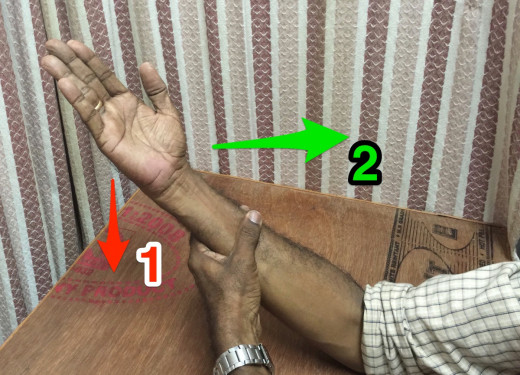
Exercise- Extend (straighten) the right elbow to the maximum and hold the right elbow in that maximum extended position. Now the patient holds his right forearm with his left hand in such a way that the fingers of his left hand lies on the dorsal aspect (back side) of his right forearm and his left thumb lies on the palmar aspect (front side) of the right forearm. Now the patient tries to extend (straighten) his right elbow (with the right wrist and right fingers still held extended) while a resistance is offered against the ‘straightening force’ by his left hand which is holding it.ie. The effort of the patient to straighten the right elbow is opposed by an equal and opposite force (resistance) offered by the left hand which is holding it. Hence no movement occurs at the right elbow. Hold the right elbow in that maximum extended (straightened) position for 2 seconds. Now relax. Slowly and gently reverse the direction of movement of the right elbow. Now the patient tries to flex (bend) his right elbow (with the right wrist and right fingers still held extended) while a resistance is offered against the ‘bending force’ by his left hand which is holding it. Ie. The effort of the patient to bend the right elbow is opposed by an equal and opposite force (resistance) offered by the left hand which is holding it. Hence no movement occurs at the right elbow joint. Hold the right elbow in that maximum flexed (bend) position for 2 seconds. This exercise is repeated 10 times, thrice a day.
It is to be noted that no movement occurs at the right elbow joint throughout the exercise. In other words, the right elbow remains ‘still’ throughout the exercise program. But the extensor and flexor muscles of the forearm contract isometrically.
The exercise may be repeated in the same way with the anterior aspect (front side) of the right forearm and the palmar aspect (front side) of the right hand facing downwards (with the right wrist and the right fingers held extended).

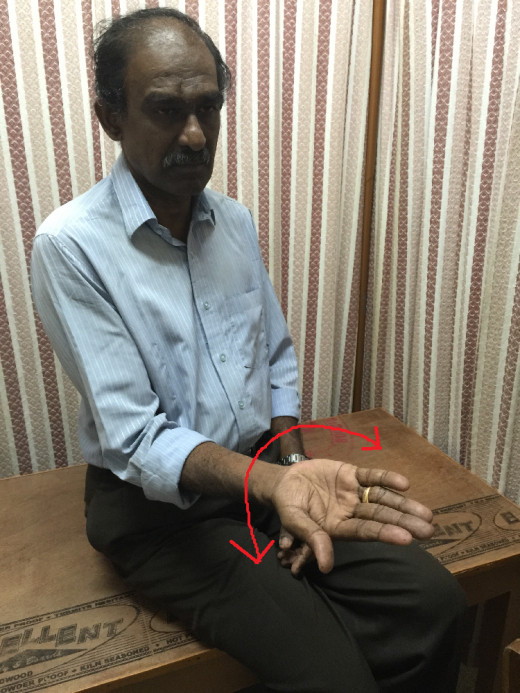
H. Hold Relax Exercise—2
Let the patient has ‘Myositis Ossificans’ in his right elbow. Let there be limitation of flexion of elbow.
Starting Position- The patient sits on a chair near a table facing it. The patient keeps his bend right elbow on the table in such a way that the elbow is bend approximately 45 degrees with the anterior aspect (front side)of the right forearm and the palmar aspect (front side) of the right hand facing upwards with the right wrist and the right fingers held extended (straightened).
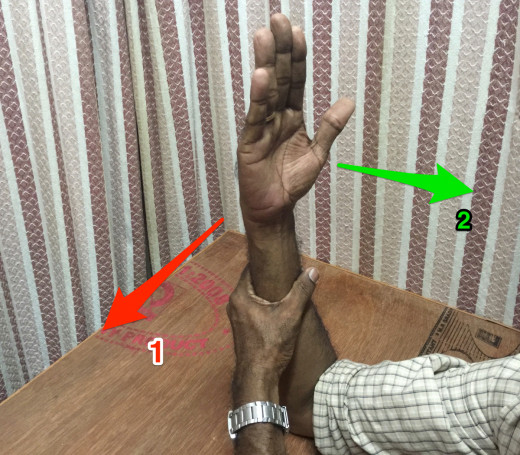
Exercise- Flex (bend) the right elbow to the maximum and hold the right elbow in that maximum bend position. The patient holds his right forearm with his left hand in such a way that the fingers of his left hand lies on the dorsal aspect (back side) of the right forearm and the left thumb lies on the palmar aspect (front side) of the right forearm. Now the patient tries to flex (bend) his right elbow (with the right wrist and fingers still held extended) while a resistance is offered by his left hand against the ‘bending force’ by his left hand which is holding it. Ie. The effort of the patient to bend the right elbow is opposed by an equal and opposite force (resistance) offered by the left hand which is holding it. Hence no movement occurs at the right elbow. Now hold the right elbow in that maximum flexed (bend) position for 2 seconds. Now relax. Slowly and gently reverse the direction of movement of right elbow. Now the patient tries to extend (straighten) his right elbow (with the right wrist and fingers still held extended) while a resistance is offered against the ‘straightening force’ by his left hand which is holding it. Ie. The effort of the patient to extend his right elbow is opposed by an equal and opposite force (resistance) offered by his left hand which is holding. Hence no movement occurs at the right elbow joint. Hold the right elbow in the maximum extended (straightened) position for 2 seconds. The exercise is repeated 10 times, thrice a day.
It is to be noted that no movement at the right elbow joint throughout the exercise program. In other words, the right elbow remains ‘still’ throughout the exercise program. But the extensor and flexor muscles of the right forearm contract isometrically.
The exercise may be repeated in the same way with the anterior aspect (front side) of the right forearm and the palmar aspect (front side) of the right hand facing downwards (with the right wrist and the fingers still held extended ( straightened)
J. Surgical Intervention
Treatment is primarily conservative as some patient’s calcification will spontaneously be reabsorbed and thus may have minimal symptoms. Occasionally surgical removal of the abnormal tissue is required. If the bone mass is not absorbed and the movements of the joint is greatly impaired the surgeon decides to remove the mass. Usually the surgical intervention is further postponed for a 6- 12 months so that the ossification is complete and the risk of its recurrence may be minimized. Even then there is a greater tendency for the surplus bone to reform as the periosteum may get further injured again during the surgical intervention. In minor cases if the presence of the bone mass does not interfere seriously to carry out the activities, surgical intervention must be avoided.
More
Related
-
Myositis Ossificans - Elbow Joint - Physiotherapy Treatment - 1
 - Upper limb")
Frenkel’s Exercises for Ataxic Conditions (Cervical Spondylotic Myelopathy) - Upper limb
 - Lower limb")
Frenkel’s Exercises for Ataxic Conditions (Cervical Spondylotic Myelopathy) - Lower limb

Isometrics for Muscle Mass: Do Isometrics Build Muscle?

20 Gross Motor Activities That Build Strength and Coordination


