Neck Pain #3 – Cervical Spondylosis (Clinical Features)


Introduction
Three main groups of symptoms are usually seen in the case of degenerative arthritis and intervertebral disc disease in the cervical spine depending upon the nature of the pressure exerted by the osteophytesand the protruded disc. It also depends upon the structures that are impinged upon.
Classification of Symptoms
1. Symptoms due to the pressure of osteophytes or central disc protrusion on the spinal cord. Cervical spinal cord compression due to the osteophytesor due to central disc protrusion is a very serious condition. Usually, it occurs at the C5 – C6 level. This condition exhibits various types of symptoms. The most important symptoms are –
- Symptoms involving upper motor neurone lesion findings in one or both lower limbs.
- Symptoms involving lower motor neurone findings in one or both upper limbs.
- Sensory disturbances in the upper and lower limbs.
- 2. Symptoms due to the pressure of osteophytes or lateral disc protrusion on the vertebral artery.
2. Vertebral artery compression due to osteophytes or lateral disc protrusion can lead to the following –
- Brainstem Ischemia.
- Vertigo.
- Tinnitus.
- Visual Disturbances.
- Difficulty in speech and swallowing.
- Ataxia and other signs of cerebellar dysfunction.
3. Symptoms due to pressure of osteophytes or posterolateral protrusion on the spinal nerves.
Cervical nerve root compression due to pressure of osteophytes or posterolateral disc protrusion on the spinal nerves is the commonest. Cervical nerve root compression usually produces pain and sensory disturbances in the distribution area of the concerned nerve root. Any way this pain and sensory disturbances may be wider spread beyond the concerned distribution levels.
Symptoms Due To Nerve Root Involvement
The symptoms due to the pressure of osteophytes or posterolateral disc protrusion on the
spinal nerve roots are the commonest. Cervical root compression usually produces pain and sensory disturbances in the distribution area of the concerned nerve root. The pain and sensory disturbances may be wider spread beyond the concerned distribution levels.
Herewith we deal with the symptoms and clinical features in the case of nerve root involvement.
- Weakness of Muscles – Involvement of motor nerve roots may cause weakness of muscles that are supplied by the concerned nerve roots. The muscles supplied by the most commonly involved roots are as follows –
- Deltoid– C5, (6)
- Biceps – C (5), 6
- Triceps – C (6), 7, (8)
- Wrist and fingers extensors and flexors – C7, 8
- Thumb abductors and extensors – C (7), 8
- Intrinsic hand muscles – C8, T1
- All muscle tests may be performed with the patient in a comfortable position, so that the muscles to be tested may be isolated. The actions of other muscles or other groups of muscles with varying nerve supply may be avoided or minimised.
- Example – The triceps may be tested with the patient supine and arm held vertically up. In this position the scapular muscles are fixed, allowing the triceps to be isolated. In this position the triceps can be easily tested for strength and for endurance.
2. Neck Rigidity – There will be limitation of neck movements. Usually the extension and rotation of the neck to the involved side is limited.
3. Pain and Paraesthesia - Aggravated by coughing and sneezing.
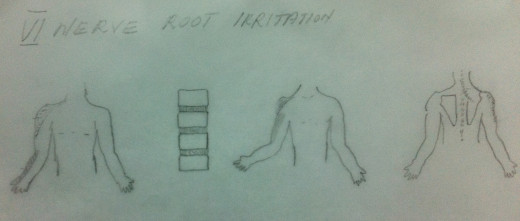
- C5 level – Usually there may be no paraesthesia.
- C6 level – Paraesthesia and Hypaesthesia of thumb and some portions of index finger.
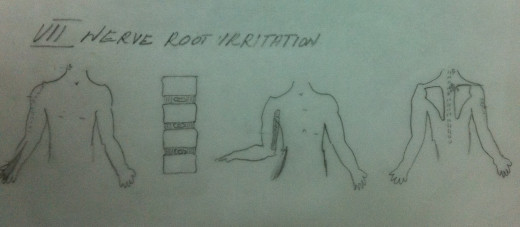
- C7 level – Paraesthesia and Hypaesthesia of index and middle fingers.
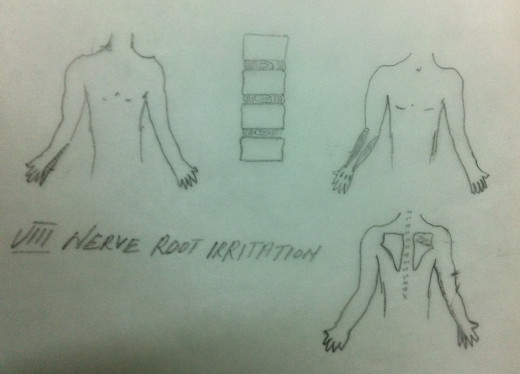
- C8 level – Paraesthesia and Hypaesthesia of inner forearm and little finger.
4.Tenderness
- C5 level – Tenderness over the exit of C5 nerve root
- C6 level – Tenderness over the exit of C6 nerve root and over deltoid and rhomboid.
- C7 level – Tenderness over the exit of C7 nerve root and over the dorsolateral upper arm and superior medial angle of scapula.
- C8 level – Tenderness over the exit of C8 nerve root, from scapula down the inner side of upper arm, inner forearm, to little finger.
5. Referred pain
- C5 level - Shoulder and upper arm.
- C6 level – Radial aspect of forearm.
- C7 level – Dorsal aspect of forearm.
- C8 level – Ulnar aspect of forearm.
6. Reflexes
- C5 level – Diminished biceps jerk.
- C6 level – Diminished biceps jerk.
- C7 level – Diminished triceps jerk.
- C8 level – Usually no reflex changes.
7. Involvement of upper functional unit ( occipito – atlanto – axial )
Hypaesthesia, Hyperaesthesia or Anaesthesia in the scalp area due to pressure or irritation of the C1, C2 nerve roots.
8. The motor nerve supply to the muscles of the inter scapular region is as follows.
- Lavetor Scapular Muscles – C3 – C4.
- Rhomboids Muscles – C5.
- Supra Spinatus Muscles - C5 – C6.
- LatissmusDorsi Muscles – C6 – C7.
- Involvement of the above mentioned nerve roots may cause motor and sensory deficiencies in the muscles concerned.