Neck Pain – Cervical Spondylotic Myelopathy


Introduction
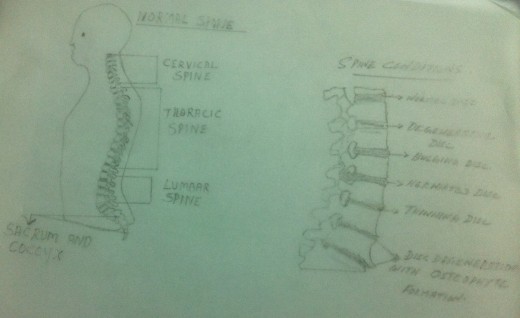
One of the most common neck problems that occur with age is Cervical Spondylotic Myelopathy. The degenerative changes of the intervertebral discs and the posterior facet joints due to aging can lead to the narrowing of the spinal canal. The narrowing of the spinal canal is called ‘spinal stenosis’.The narrowed spinal canal compresses or squeezes the spinal cord and hence the symptoms. The Cervical Spondylotic Myelopathy is presented with variety of symptoms including pain, numbness and weakness of muscles. Usually this condition is noticed in the elderly people. But it can also occur in the earlier stages if there is a history of an injury to the cervical spine at a younger age. Usually there will be a steady progression of the disease condition. Once the symptoms appear, they tend to continue. But the condition progresses slowly over several years. But in some cases the condition worsens more rapidly.
Knowledge regarding the cervical spine and its function is helpful in understanding the Cervical Spondylotic Myelopathy better. Please refer my earlier article ‘Cervical Radiculopathy’ for details regarding the ‘Anatomy of the Intervertebral Disc’, ‘Degenerative Changes of the Intervertebral Disc’ and ‘Herniated Disc’.
What is Cervical Spondylotic Myelopathy?
Cervical Spondylosis affects the width, height and shape of the intervertebral foramina and the spinal canal. As a result the spinal canal gets narrowed and is called ‘spinal stenosis’. ‘Stenosis’ of the spinal canalcompresses and squeezes the spinal cord and hence the symptoms. The spinal cord fills four – fifth of the spinal canal and is held in taut by the ‘dentate ligament’.(This ligament is a broad band of piamater projecting as longitudinal fin from each side of the spinal cord. It lies between the ventral and dorsal roots and get attached laterally to the duramater which lines the canal). This ligament limits the excessive motion of the cord within the spinal canal.
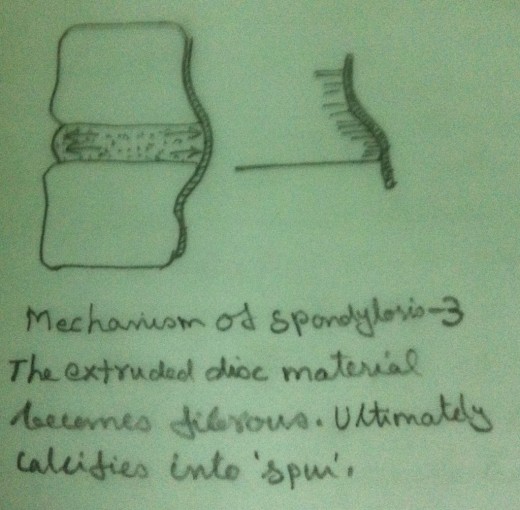
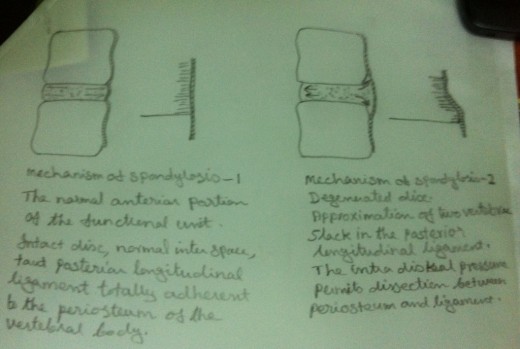
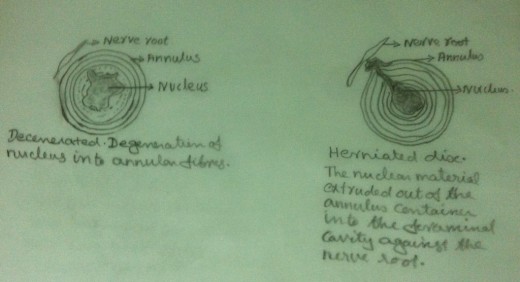
Any encroachment to the canal due to bulged or herniated disc, osteophytes, spurs, cyst, tumour or abscess can cause compression of the spinal cord. Cord involvement causes cord myelopathy with upper motor neurone signs and symptoms. In the case of Cervical Spondylotic Myelopathy, the compression of the cord occurs usually from osteophytes in the anterior portion of the functional unit and from the degenerative cartilage changes in the posterior facet joints. There may be a congenital factor also in the narrowing of the canal.
Causes for Cervical Spondylotic Myelopathy
- Bulged or Herniated Disc
- Vertebral Subluxation
- Osteophytes or Spurs due to degenerative changes in the disc or in the facet joints
- Acute angulation of Cervical Spine
- Traumatic injury to the cervical spine from motor accidents
- Acute or sustained hyperextension of the neck from an injury or after a lengthy dental procedure.
- Osteoporosis of the Cervical Spine due to aging
- Congenital abnormalities of Cervical Vertebrae
Causes for Cervical Myelopathy
- Cysts
- Tumours
- Abscess
- Infections
- Ischemia - deficiency of blood supply due to vascular diseases.
- Autoimmune diseases such as Rheumatoid Arthritis, Multiple Sclerosis, Transverse Myelitis etc.
- Jobs or Sports involving regular and continuous stretching or straining of cervical spine.
Investigations
- Clinical Examination
- Motor Examination – There may be Weakness of Muscles.
- Sensory Examination – There may be Sensory Deficiencies.
- Evaluation of Reflexes – Usually Hyperactive
- Evaluation of Range of Motion – Usually Restriction of Movement
- Evaluation of Co-ordination – Incoordination present.
- X ray Evaluation
- CT Scan
- MRI
- EMG
- Nerve Conduction Test
- Somatosensory Evoked Potential Test
- Visual Evoked Potential Test
Signs and Symptoms
- Sensory Deficiencies – Feeling of numbness and tingling in the arms and the legs - a feeling of discomfort and light handedness in the arms, hands, legs and trunk – hypersensitivity of hands and feet, impairment of temperature sensation and impairment of vibration sensation.
- Motor deficiencies – Weakness of upper limbs and lower limbs, weakness of the small intrinsic muscles of the hand or hands (the weakness may be unilateral or bilateral, sometimes only the upper limbs are involved, sometimes only the lower limbs are involved or sometimes all the four limbs are involved).
- Reflexes – Abnormal reflexes – usually hyperactive (hyper- reflexia).
- Pain – Pain is usually insignificant – But present if there is related nerve root entrapment due to foraminal stenosis. In such cases there may be radiating pain also.
- Co-ordination – There may be incoordination of movements of upper limbs or lower limbs (unilateral or bilateral) – there may be impairment of fine hand movements.
- Atrophy – There may be atrophy of muscles of the limbs especially the intrinsic muscles of the hands in the case of nerve root involvement.
- Limitation of range of motion –There may be limitation of range of motion of cervical spine.
- Gait disturbance – There may be difficulty in balancing – unsteady gait with wide base.
- Bladder Dysfunction
Points to remember
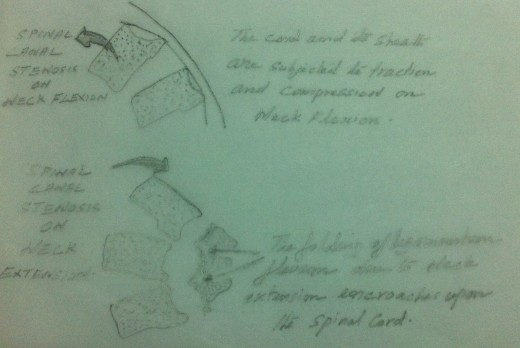
- In forward flexion, in the presence of Cervical Spondylosis, the cord and its dural sheath are subjected to traction and compression and thus decrease the width of the spinal canal. It increases the pressure on the cord and hence aggravates the symptoms.
- The symptoms of Cervical Myelopathy often begin insidiously and progress slowly. A gradual onset of Cervical Myelopathy may occur with no radicular symptoms and with minimum X- ray evidence of degeneration. Conversely, there may be severe spinal degenerative changes with no central nervous system involvement or impairment.
- Both in flexion and extension of the cervical spine, there may be folding of ligamentumflavum. This results in the encroachment upon the contents of the spinal canal and aggravates the symptoms.
- Damages to the spinal cord and the symptoms there from depend upon the specific tract or tracts (specific areas) of the spinal cord which is compressed upon. Hence the symptoms are likely to vary from patient to patient.
- Whether the damage to the spinal cord is caused from mechanical pressure due to degenerative changes in the cervical spine or due to vascular impairment is immaterial as for as the symptoms are concerned.
Surgical Treatment
Whether surgery is to be done or not is a complex decision. If there is structural pressure on the spinal cord, surgery is indicated.
- Discectomy- A surgical procedure to remove part of an intervertebral disc that is putting pressure on the spinal cord or nerve root.
- Laminectomy- A surgical procedure to remove a portion of a vertebra, the lamina.
- Fusion of the vertebrae- A fusion surgery fuses two or more vertebrae in to one solid bone. After discectomy, the disc space is filled in with a small block of bone graft. The bone is allowed to heal fusing the two adjacent vertebrae in to one solid bone.
Non-Surgical Treatment – Medications
- Non-Steroid Anti Inflammatory Drugs.
- Oral Corticosteroids.
- Epidural Steroid Injections.
- Narcotics.
- Muscle Relaxants.
- Anti-Spastic Drugs.






