No Natural Cures For Ovarian Cysts

The title is provocative and deliberately so. It is important that snake-oil salespeople are confronted and exposed. This is one area where they have thrived, exploiting other people’s discomfort to plump their wallets. If this hub saves one victim from their clutches, it will be worth it.
A couple of days ago I did a specified Google search for natural cure for ovarian cysts. It returned 1.2 million results! Of course it is possible some of those are there to educate and debunk fraudulent claims but it is safe to assume many, probably most, will be promoting some brave new world of ‘natural shrinkage and elimination of cysts’
Understanding cysts
A cyst is a collection of fluid inside a sac, usually arising from an organ such as the ovary. Cysts can be found in many parts of the body including the liver, kidneys, limb joints and even the brain. They can really arise anywhere in the body. The cystic fluid could be watery clear, viscous, bloody or mucous.
The Pill

Functional ovarian cysts
The first and probably most important thing one needs to know about ovarian cysts is that the vast majority are not abnormal. The second important point is that most of them are transient. Let’s explore these two points further.
The ovaries of any woman in a child-bearing age do form cysts. It is part of their biological function. Every four weeks, give or take a few days, eggs go through a process of maturation. That involves formation of what is called a corpus luteum cyst. Normally, once the egg has been released (ovulation), the cyst will gradually shrink and resolve only to be replaced by a new one in the next cycle. This process is repeated every month for the most part of the 30 years or so that a woman spends in the so-called child-bearing age. The only times this does not happen is if she is on a hormonal contraceptive, is pregnant or is fully breast feeding. Also; there are conditions and medications which interfere with this normal physiological process.
Corpus luteum cysts can be persistent. Whilst in most cases the corpus luteum cyst resolves, in some cases the cysts persist and could remain in place for several months. A typical persistent corpus luteum cyst is unilateral (found on one side only), does not change in size and remains painless. They almost invariably resolve spontaneously but duration of persistence varies a great deal.
Follicular cysts are another type of ‘functional’ cysts. They develop when ovulation does not follow maturation of the follicle. Let me explain. Ovaries have hundreds of thousands of eggs within. Every month, a few start the process of maturation. Only one will usually be released in each cycle. One or two other follicles which started the process of maturation but from which the egg is not released may go on to form cysts which are usually small or moderate in size, rarely exceeding 5cm in diameter. On ultrasound scan they are round with a thin membrane forming the sac and typically clear fluid (which appears uniformly black on scan). Occasionally such a cyst will rupture causing sharp localised pain which tends to resolve within an hour or two but can persist as a dull ache for several more hours. Cystic rupture is uncommon. Sometimes bleeding occurs within a follicular cyst. This will change the scan appearance. The cyst is then classified as ‘haemorrhagic’. These can cause pain, which, again is transient. A haemorrhagic cyst can persist for weeks but the preferred management is still conservative as these too, invariably resolve.
Ovarian dermoid

Dermoid Cysts
A dermoid cyst is not functional. These types of cysts result from a developmental mishap during the fetal stage. A dermoid cyst is a benign growth that is largely cystic. We say ‘largely’ because a dermoid cyst always contains various types of tissue other than fluid. Commonly found within a dermoid cyst are such structures as teeth, hair and skin. You can also find cartilage, nails, thyroid tissue and all sorts of other tissue. What is important to know is that a dermoid cyst is present at birth and only grows very slowly. Discovery is usually incidental when a woman is having a scan for an entirely unrelated reason. Many are discovered during routine pregnancy scans. Ovarian dermoid cysts are almost always symptomless but can grow to sizes which create a risk of torsion (twisting). When a dermoid cyst becomes rather large (over 5 cm diameter), the risk of it twisting on its stalk is increased. If this was to happen, it will create a surgical emergency because the torsion will compromise or cut-off the blood supply to the ovary causing acute pain. Only surgery can undo the torsion. Dermoid cysts are also known by the name ‘mature cystic teratoma’. Removal of uncomplicated dermoid cysts is not mandatory being overwhelmingly benign and symptomless. However, if it is desired or necessary to remove a dermoid cyst; surgery is the only option.
What many may not realise is the fact that the ovary is not the only site for dermoid cysts. They are also found on the face (usually dealt with in childhood), lower back, in the brain and spinal cord (rarely) and other parts of the body.
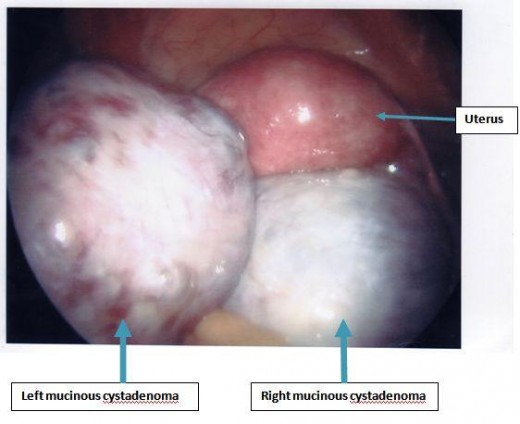
Cystadenoma
These are benign cystic tumours which arise from ovaries. The growth can be progressive and some of these can grow to enormous sizes extending from the pelvis into the higher reaches of the abdominal cavity. There are two broad types on the basis of the type of fluid they contain. . The serous cystadenoma contain watery, usually lightly straw-coloured fluid. Mucinous cystadenomas contain mucous type fluid as the name suggests. The cells lining the wall of the cyst are responsible for secreting the fluid. Even though these are benign and in most cases painless, the case for surgical removal is based on their ability to grow and attain large sizes with all the attendant problems associated with that.
Bilateral ovarian cysts
Malignant cysts
The cystadenomas mentioned above have got malignant cousins which a lot less common. These go by the names ‘serous cystadenocarcinoma’ and mucinous cystadenocarcinoma’. Imaging investigations (ultrasound, CT scan and MRI) will usually distinguish between the benign and the malignant.
Endometriotic cysts
People with the rather common condition ‘endometriosis’ can develop cysts on the ovaries arising directly from the condition. The endometriotic cysts also go by the name ‘endometrioma’. They are also known by the acronym ‘chocolate cysts’ which comes from the fact that the contents of the cysts are thick dark brown old blood similar to chocolate mousse. Whilst there is effective medical treatment to control the underlying condition (endometriosis), once an endometriotic cyst has developed, it can only be removed surgically.
PCOS
. The numerous small round cysts (appearing black) can be seen 'surrounding' the ovary. It is this finding that gives the condition its name 'polycystic'")
Polycystic ovaries
This condition is mentioned here only for clarification. Ovaries in polycystic ovarian syndrome (PCOS) do not contain cysts in the true sense of the word or as described above. The ovaries in this condition contain numerous tiny cysts usually in the periphery which are the hallmark of the condition. The tiny cysts are actually not the cause of the condition; they are just a manifestation. As such, they don’t go away, are not amenable to surgical removal (which will be pointless anyway), do not increase in size and, in themselves; do not cause any problem. A cyst in PCOS measures no more than a couple of millimetres in size.
Not a monolithic condition
So, there you have it. You can see that there is a whole variety of cysts with a whole range of underlying causes. If you read the ‘literature’ that promises a natural cure for ovarian cysts, there is usually a broad-brush mention of ‘hormonal imbalance’ as if this is the one chief cause of cysts (hogwash!) and why the remedy will enable you to avoid surgery (you most likely never needed it in the first place). If you have to take away a few facts from this hub, please let that be:
- Ovarian
cysts are common and can occur at any age but are commonest in the child-bearing
years.
- Ovarian cysts should not always be regarded as abnormal. Functional cysts (the commonest) are perfectly natural. They come and go.
- Not all ovarian cysts are the same. There is a wide variety of underlying causes.
- Use of the oral contraceptive pill, by abolishing the menstrual cycle, reduce the probability of developing functional cysts.
- Most ovarian cysts are functional and have a life span ranging from a few days to a few months.
- Functional cysts are almost always painless and resolve spontaneously in due course. Treatment is very rarely necessary.
- If you have pelvic pain and a scan shows an ovarian cyst, it may not be responsible and odds are, it is not. Concentrating on that may waste valuable time and resources.
- Dermoid cysts are not functional but are almost always benign. If treatment is required, a dermoid cyst has got to be surgically removed. No medication can effect ‘resolution’ of a dermoid cyst.
- When benign cysts attain a large size, they carry a risk of torsion which creates a surgical emergency.
- Cysts associated with endometriosis (endometriomas) can only be treated surgically.
- Large cysts are usually benign but possibility of malignancy should always be borne in mind and appropriate blood and imaging investigations carried out to clarify the status.
This content is for informational purposes only and does not substitute for formal and individualized diagnosis, prognosis, treatment, prescription, and/or dietary advice from a licensed medical professional. Do not stop or alter your current course of treatment. If pregnant or nursing, consult with a qualified provider on an individual basis. Seek immediate help if you are experiencing a medical emergency.
")






