The Health Significance And Clinical Manifestations Of Nonveneral Treponematoses (Yaws And Pinta)

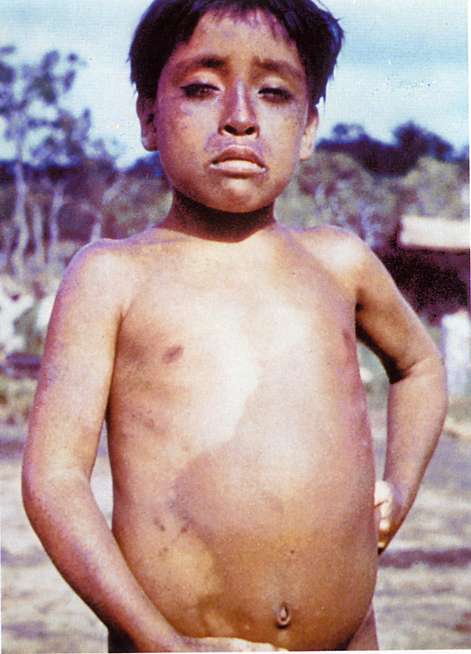
The Physical Presentations Of Yaws

Yaws
Yaws and pinta are non-veneral diseases caused by spirochetes which resemble Treponema pallidum morphologically and epidemiology. Primary infection is usually acquired in childhood. Transplacental transmission of infection does not occur usually. Pathologic lesions are confined to the skin and bones, the other viscera are not affected as in syphilis.
Yaws
Yaws is widely prevalent in the tropics and subtropics. It is seen sporadically in all parts of India, though the disease is more prevalent in Africa. The causative organism is treponema pertenue. The discharges from the primary and early secondary lesions teem with the organism. Portal of entry is abrasions on the skin. Overcrowding and poor personal hygiene favour transmission. Three stages: primary, secondary and tertiary can be indentified during the course of the disease. With the improvement in living conditions and advent of penicillin therapy, the picture of yaws and its prevalence have changed considerably, though there are some suggestions that the disease is also showing signs of resurgence.
The primary stage: This shows red maculopapular lesions which develop at the site of inoculation of the organism after three to six weeks. These enlarge and become multiple. They are painless but pruritic. Ordinarily, they heal without scarring.
The secondary lesions: develop in crops, weeks to moths after the healing of the primary lesions. Though they resemble the primary lesions, they are more numerous and widely distributed over circumoral, axilary, perineal and perianal regions. In the moist areas, they assume the appearance of condylomas. Over the palms and soles, the lesions become painful and walking may be restricted due to pain (crab yaws). Bones are affected in the secondary stage. Multiple long bones are involved. The shaft shows cortical rarefaction and subperiosteal inflammation and new bone formation. The affected part is thickened and painful. Nasal bones show thickening (gondov) and the tribial lesion may give rise to sabre tibia.
The tertiary stage develops 5 to 10 years later with gummatous and destructive lesions. The skin and bones are affected. Deep ulcers develop which show overhanding edges. Chronic destructive lesions in the bone may lead to discharging sinuses. Extensive destruction of the facial tissues with gross formation of a single open cavity (gangosa).
Diagnosis: Clinical suspicion should be strong to diagnose this condition since it occurs sporadically or in families and the condition is likely to be missed by the unwary physician. Yaws has to be differentiated from other granulomatous lesions involving the skin and bones such as syphilis, tuberculosis, leprosy and mucocutaneous leishmaniasis. The diagnosis is confirmed by demonstrating the treponemes in the discharges from primary and secondary lesions by dark ground illumination. Serological tests resemble those of syphilis.
Treatment: Dramatic improvement occurs with a single dose of 1.2 mega units of benzathine penicillin given intramuscularly. An alternative regimen is to give tetracycline 1- 2g daily for 5 days. Early cases are cured, whereas in the late cases, mutilation may persist.
The Physical Presentation Of Pinta
Infectious Diseases

Pinta
Pinta, which is also a non-veneral treponemal disease prevalent in South and Central America, is caused by Treponema Carateum. Transmission occurs by close physical contact and the organism enters through skin abrasions. Exudates from the early skin lesions are highly infective.
Clinical features: The incubation period is 7 to 12 days. The primary lesions develop at the site of inoculation as erythematous, pruritic papules, which coalesce to form ulcers, which take a long time to heal. Scarring and depigmentation occur at these sites.
The secondary stage develops three to twelve months after the primary stage. Morphologically, these lesions resemble the primary lesions. They are smaller but more numerous and widely distributed. Lesions at different stages of development occur simultaneously. Constitutional symptoms may occur at this stage. When the skin lesions heal, atrophy, scarring and depigmentation result.
Diagnosis: The discharges from early skin lesions reveal spirochetes on dark groun illumination. In late lesions organisms may not be demonstrable. Serological tests for syphilis are positive in such cases.
Treatment: Single dose of 1.2 mega units of benzathine penicillin given intramuscularly is curative in most of the cases.
© 2014 Funom Theophilus Makama