Vesiculo- Bullous Eruptions: Lyell’s Syndrome, Dermatitis Herpetiformis And Erythema Multiforme

Toxic Epidermal Necrolysis (Lyell’s Syndrome)
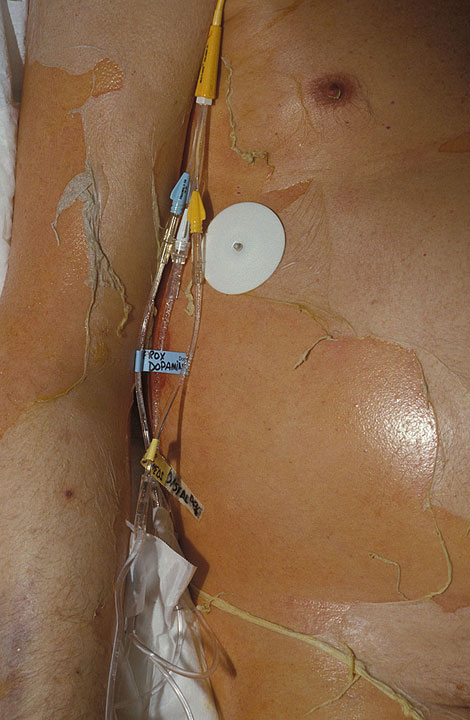
Toxic Epidermal Necrolysis (Lyell’s Syndrome)
These scary-named diseases are special kinds of skin diseases resulting to the creation of vesicular or bullous lesions on the skin and may even cause more damages. What are their significance to Man’s health?
Toxic Epidermal Necrolysis (Lyell’s Syndrome)
This is an acute bullous lesion caused by epidermal separation characterized by the presence of bullae similar to those seen in scalding. The mucocutaneous junctions are affected more. Constitutional symptoms such as fever are present. It is a manifestation of drug allergy in many cases. Drugs such as phenacetin, barbiturates, penicillin, sulphonamides and many others may be responsible. Some authors attribute toxins of staphylococci to play an etiological role. The bullae are flaccid and Nickolsky’s sign is strongly positive. Principles of management include hospitalization, removal of the cause, and attention to general health. Infection and electrolyte disturbances have to be attended to.
Dermatitis Herpetiformis

Dermatitis Herpetiformis
This is a chronic relapsing dermatitis characterized by severe pruritis and polymorphic lesions occurring in clusters. Adult males are affected more than females. There is a distant form which affects children. The etiology is not clearly understood. Pathological changes are seen mainly in the dermis. These include vascular dilatation, edema and infiltration by eosinophils and lymphocytes predominantly. The bullae are sub-epidermal.
Clinical features: The onset is usually sudden. Prodromal symptoms such as malaise may be present. The site of lesion becomes pruiritic and painful and polymorphic, bilaterally symmetrical vesicular and bullous lesions appear in crops. Along with these, other lesions such as reddish plaques (erythematous macules) and pustules may also appear. The scapular region, lumbosacral region, buttocks and forearms are the sites of predilection. With the onset of vesiculation, the pruritus comes down. As the vesicles subside, crusting, scarring and pigmentation follow. It is only rare that mucous membranes are affected. About 70% of the cases are associated with small intestinal disturbances. Unlike as in pemphigus vulgaris, systemic disturbances are minimal.
Diagnosis: Diagnosis is essentially clinical. Some cases may resemble pemphigus vulgaris. The distinctive features have been summarized in a table in the previous hub, just click on the previous hub on the slide below. The course of dermatitis herpetiformis is chronic with a fluctuating pattern. Life is not shortened, but some cases may develop pemphigus on long follow up.
Treatment: General management consists of rest, removal of septic foci and antibodies if required.
Specific therapy: Dapsone in a dose of 50 mg/day and sulpharyridine in a dose of 2 to 3 g/day bring about excellent response. Local application of antipruritic lotions like 1^ phenol in calamine lotion gives symptomatic relief.
Erythema Multiforme


Erythema Multiforme
In the tropics, this is a less common lesion but it is frequent in the temperate zones. Probably, the condition results from sensitization by infective agents, eg. Streptococcus hemolyticus or drugs. In many cases, there is a previous history of sore throat or drug intake.
Clinical features: The onset is acute with general symptoms like fever and malaise. The skin lesions are multiple and polymorphic, distributed symmetrically over the dorsum of the hands and legs, face and neck. The skin lesions consists of edematous maculates and flatterned papules. Vesiculation is uncommon. At times, bullae may develop. Such bullae arise from erythematous bases. Mucous membranes are not generally involved. The local lesion is asymptomatic except for mild pruritus or burning. Rarely, erythema multiforme may be associated with gastrointestinal upsets, arthritis or hemorrhages.
Stevens Johnson Syndrome: This is a severe form of erythema multiforme in which extensive bullous lesions occur in the skin and mucous membranes of the mouth, eyes, urethra and respiratory tract. This is associated with high fever and prostration.
Course and prognosis: The whole attack of erythema multiforme lasts for 2 to 4 weeks. Recurrence is not uncommon. Majority of cases heal spontaneously if the offending agent is removed by the bullous variety can be severe and even fatal.
Principles of treatment: (a) withdraw the offending agent such as drugs or dietary allergies, (b) infections are treated with appropriate antibiotics, (c) antihistamines given orally reduce the severity of the attack, (d) in severe cases, corticosteroids are indicated, (e) local relief can be obtained by application of calamine lotion containing 1% phenol.
Conclusion
Though. Toxic epidermal necrolysis, dermatitis herpetiformis and erythema multiforme could be very uncomfortable during their manifestations, they still stand a very low risk to life and are highly treatable.
© 2014 Funom Theophilus Makama

: Symptoms, Causes, and Treatments")





