Visceral Leishmaniasis: Health Implications, Epidemiology, Pathology And Transmission

Various clinical Presentations Of Visceral leishmaniasis

Visceral Leishmaniasis (Kala-azar)
This is a prolonged febrile illness associated with progressive emanciation, anemia and hepatosplenomegaly caused by Leishmania donovani which parasites the reticuloendothelial cells in the spleen, liver, bone marrow and other viscera. This disease has been in existence in places like India for over a hundred and fifty years. On one occasion was in Bihar in 1977 and 1978 in which more than 60,000 people suffered. The name Kala-azar (black fever) is derived from the dark pigmentation that develops in the victims of visceral leishmaniasis. The parasite (L.D. body) was discovered in 1903 simultaneously by Leishman in England and Donovan in Madras.
Epidemiology Of Kala-azar
Apart from several states in India, the disease is present in East and North Africa, Sudan, Bangladesh, parts of China and Russia, South Iran, Arabia, Mediterranean countries of Europe, Ethiopia, Kenya and South America, including Brazil and Venezuela. In India, the disease is most endemic in the eastern half, but isolated pockets exist in almost all regions from where sporadic cases and even small outbreaks have been reported from time to time. The conditions conducive for the development of the vector are: altitude below 700m, high rainfall and humidity, alluvial soil, abundant vegetation and a rural setting.
In the Mediterranean region, infants and children are almost exclusively affected. In other endemic areas including India, though the disease is more frequent in children and the young, older age groups are also susceptible. Males are affected more than females. Kala-azar is more prevalent in rural settings where conditions exist for the multiplication of the main vector sandfly- Phlebotomus angentipes. Only females act as vectors. It is possible that Phlebotomus papatasi also transmits the disease.
In India, Kala-azar is a disease of humans and animal reservoirs are not reported. In other endemic areas, dogs and rodents have been identified as suffering from the disease and these contribute a natural reservoir from which man is affected.
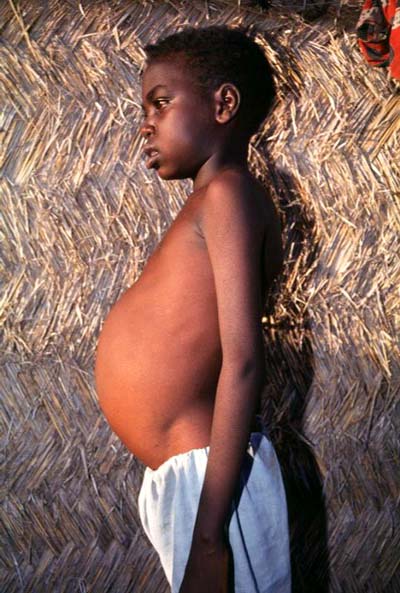
Splenomegaly In Visceral Leishmaniasis

Transmission And Pathology Of Visceral leishmaniasis
Transmission
Amastigotes of L. donovani reach the stomach of sandflies while sucking blood from infected persons. The parasite develops into flagellates (promastigotes or leptomanad form) in the midgut of the vector and within 5 to 7 days, the organisms multiply heavily and extend anteriorly to the proboscis. With the next blood meal, the promastigotes in its proboscis and pharynx are introduced into the bite wound. In the dermis, the promastigotes become amastigotes and these are taken up by the cytoplasm of the macrophages and when the host cells rupture, they are liberated into the tissue spaces. These are taken up by other macrophages and further proliferation occurs. Foci of parasitic multiplication comprising of parasitized macrophages, histiocytes and lymphocytes are formed. The parasitized reticulo-endothelial cells from these foci, pass into the circulation to reach several organs and lead to visceral infection.
Pathology Of Visceral Leishmaniasis
In the mammalian hosts, the parasite is almost exclusively restricted to the cells of the mononuclear phagocyte system (RE cells). In the visceral form, the parasites are seen in the phagocytic cells of the liver, spleen and bone marrow. In the cutaneous form, these are seen in skin macrophages. Most conspicuous changes are seen in the spleen, the liver and the bone marrow. The spleen is moderately enlarged and soft in an average case, but occasionally it may become very large an firm. Splenic infarcts and perisplenitis may occur in very chronic cases. Malpighian corpuscles are atrophic. Macrophages containing L.D bodies are seen in large numbers in the splenic pulp. Plasma cells, histiocytes and lymphocytes are seen in large numbers in the elsions. Extramedullary hematopoiesis may be present at times.
Their liver is enlarged, pale and shows fatty changes. Histology shows the Kupffer cells distended with L.D bodies, vascular congestion and fatty changed in the hepatocytes. The portal tracts show cellular infiltration and parasitized macrophages. The bone marrow becomes hyperplastic. Yellow marrow in the shafts of long bones is replaced by cellular red marrow. Parasitized macrophages are seen in large numbers in the R.E cells. Plasma cells may be increased. At times, the lymph nodes, adrenal cortex and the interstinal mucosa may show parasites within macrophages. Lymph node involvement is more characteristic of the African and Mediterranean varieties.
© 2014 Funom Theophilus Makama

")



