Vitamin D Deficiency (Nutritional Rickets And Osteomalacia): Nutritional And Health Significance And Diagnosis

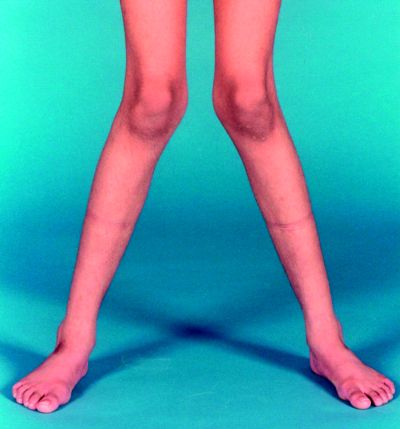
Physical Presentation Of Rickets

A General Overview
Vitamin D is required for normal metabolism of calcium and phosphorus and for bone formation. It enhances the absorption of these minerals from the gut, their mobilization from bone and the reabsorption of phosphorus by the kidney.
The two different forms of vitamin D active in man are vitamin D2 (calciferol), obtained by ultraviolet irradiation of ergosterol which is of plant origin and vitamin D3 (cholecalciferol) which is formed by activation of 7- dehydrocholesterol present in human skin as a pro-vitamin D2. This activation is effected by the ultraviolet rays of the wavelength in the range of 296 to 310 nm obtained from sunlight.
Vitamin D2 and D3 which are identical in potency differ in the configuration of the side chain. Dietary sources of vitamin D are milk, butter, cheese, egg yolk, and fish liver oils. This vitamin is heat stable. One international unit (IU) is equivalent to 0.025 ug. Deficiency of vitamin D causes rickets in the growing child and osteomalacia in the adult. The minimum daily requirement is 400 IU.
The highest prevalence is in China and Mongolia, where up to 50% of children have serum 25-hydroxyvitamin D levels

Rickets
Prevalence
Ricckets is prevalent in India, more so in the north than in the south. Premature babies are more vulnerable. The disease is more florid during winter months when exposure to sunlight is minimal Prevalence is more among the poor and illiterate classes. Indians who have emigrated to affluent countries still show a higher prevalence of rickets. Osteomalacia is more common in multiparous women who have nursed their babies repeatedly.
In rickets, the arrangement and normal degenerative processes of cartilage are abnormal. Subsequent calcification of the cartilageinous matrix and osteoid do not proceed normally. The osteoid and cartilage which remain uncalcified are deposited irregularly. These give rise to a wide irregular frayed zone of non-calcified cartilage and osteoid termed rachitic metaphysic. These in turn account for many of the skeletal deformities. In the sub-periosteal region also, while resorption of cortical bone continues normally, new bone is not laid down, resulting in softening and rarefaction of the bone shaft.
In vitamin D deficiency, since absorption of calcium and phosphorus from the gut is defective, serum calcium and phosphorus levels fall. Lowered level of serum calcium stimulates the secretion of parathyroid hormone which, in turn, leads to mobilization of calcium from the bone. Thus, the serum calcium is usually maintained normal for considerable periods, tetany developing only rarely. Since parathyroid hormone (PTH) decreases reabsorption of phosphorus by the renal tubule, the serum phosphorus falls. The serum alkaline- phosphatase is elevated due to increased osteoblastic activity.
Physical Presentation Of osteomalacia

Diagnosis
Rickets should be suspected in any child showing deformities of the skull, long bones and ribs and inthose with apathy, flabbiness, delayed milestones of development, laryngysmus stridulus or convulsions.
The clinical diagnosis is supported by the history of inadequate vitamin D in the diet or chronic diarrhea interfering with absorption of vitamin D and it is confirmed by radiological investigations and biochemical tests.
X-ray findings in active rickets: Routine skiagrams of the wrists give clues in diagnosis and are helpful for following the progress. The distal ends of radius and ulna appear concave (cupping), widened (flaring) and irregular (fraying). The distance between the distal ends of the ulna and the radius and the metacarpal bones is apparently increased wince the uncalcified rachitic metaphyses is translucent to x-ray. Shafts of long bones show decreased density and prominent trabeculations. Subperiosteal osteoid may give a double contour to the shaft.
With treatment, the lesions tend to heal. A line of preparatory calcification (LPC) appears. This is separated from the distal end of the shaft by a zone of translucency caused by the uncalcified osteoid. As healing progresses, the osteoid becomes calcified and shaft apparently grows towards the LPC and unites with it.
Biochemical Changes: In florid cases, the serum phosphorus is low (1.5 to 3.5 mg/d). Serum calcium may usually be normal, but in advanced cases it is reduced especially in cases with tetany. Serum alkaline phosphatase is raised to 20 to 60 KA units/dl (Normal is 5 to 15). With correction of the lesion alkaline phosphatase level falls and serum phosphorus level goes up.
© 2014 Funom Theophilus Makama







