How back pain works?


Introduction
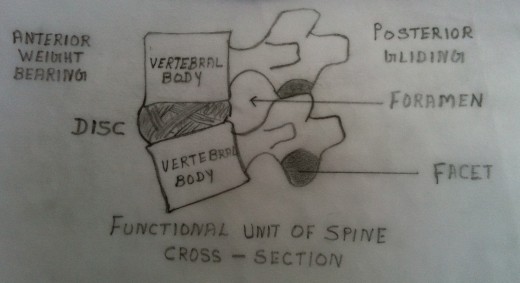
The Intervertebral discs lie between successive vertebral bodies from the second cervical vertebra downwards. They are composed of fibrocartilage. The outer portion of the disc is composed chiefly of concentric rings of fibrous tissues, the annulus fibrosus.
The annulus fibrosus is composed of layered sheets of collagen fibres. The sheet of collagen fibres reacts to tension elongation as does each individual collagen fibre. Each collagen fibre originates around the circumference of the vertebral end plate passing to the adjacent vertebral end plate at an angulation (approximately 30 degrees). The centre portion of the disc is softer and gelatinous.
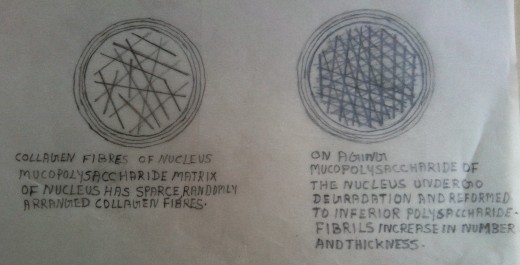
The nucleus pulposus forms the central portion of the disc. It is softer, gelatinous, homogeneous and elastic. It is centrally located within the fibrocartilaginous covering, the annulus fibrosus. The nucleus is predominantly a mucopolysacchride homogenous matrix. It contains a network of bonded fibrils layered in a random manner. These fibrils interlock each other at an approximately 60 degrees angle. This structure imparts tensile strength against deforming forces. This mechanical arrangement of the fibrils accounts for its elasticity and its tensile strength.
Physiological changes
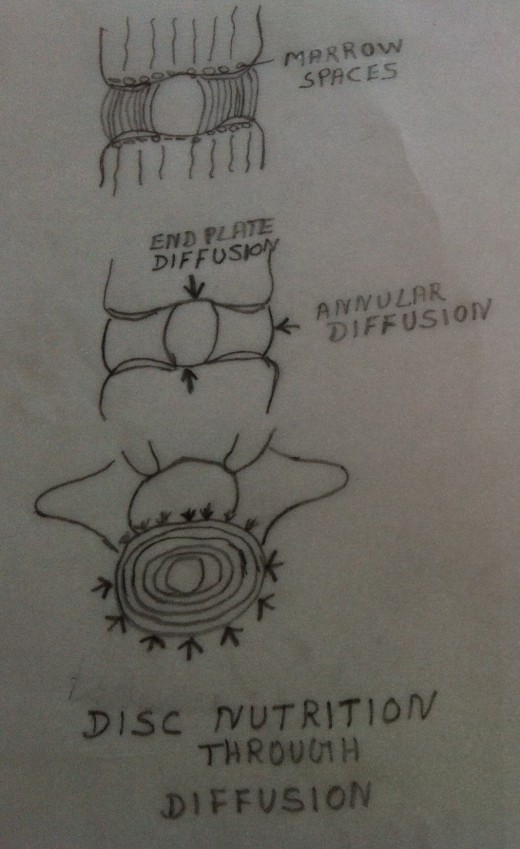
The disc in early human development is nourished by direct blood supply. The blood vessels pass through the vertebral end plates directly into the intervertebral disc. By the age of maturation, the epiphysis closes with the cessation of physiological growth. As a result the end plates calcify. The blood vessels get obliterated and the intervertebral disc becomes ischaemic. At this stage the nutrition of the disc is by “osmosis” and by “imbibition”. For “imbibition” to take place it is mandatory that there is alternating compression and relaxation of the disc to ensure its “sponge imbibition action”. Mechanically, the sponge like imbibition allows entry of fluid through the semipermeable membranes. ie. through the end plates of the vertebrae and the outer annular covering of the disc.
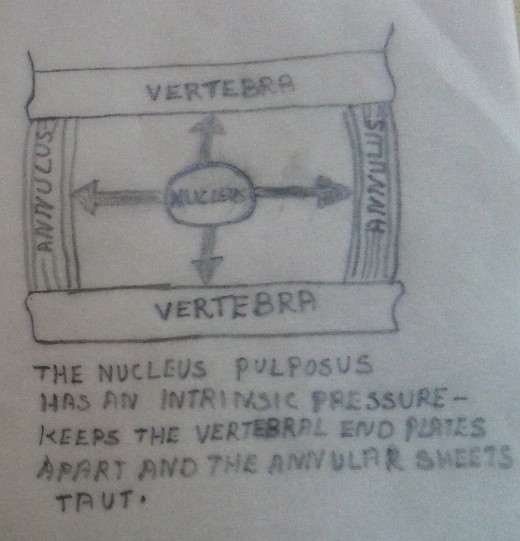
There exists an intrinsic internal pressure within the disc. This intrinsic internal pressure separates the vertebral endplates and maintains a pressure on the annular fibres. This pressure on the annular fibres keep them elongated and under a degree of pressure. Mechanically, it is apparent that the annular fibres would become slack if the intrinsic internal pressure within the nucleus dropped.
The nucleus undergoes physical and chemical changes with aging and from mechanical injuries that impair the function of the annulus. The mucopolysaccharides of the matrix undergoes degradation and they get reformed into an inferior type of polysaccharides. This degraded and reconstituted muccopolysaccharide absorbs excessive water, but cannot retain it within the matrix. Genetic, metabolic, endocrine and mechanical factors may contribute to the matrix degradation.
Mechanism of Disc Prolapse
During the early adult life the discs become avascular and degenerative changes set in followed by a reduction in water content (discussed earlier). Such degenerative changes of the disc result in extrusion of the contents of the nucleus pulposus through weakened portions of the annulus fibrosus. Such extrusion may occur through the vertebral plates into the adjacent vertebrae. These nodes are called “Schmorl’s Nodes”, which are harmless. But multiple nodes may lead to degenerative changes and will result in loss of height.
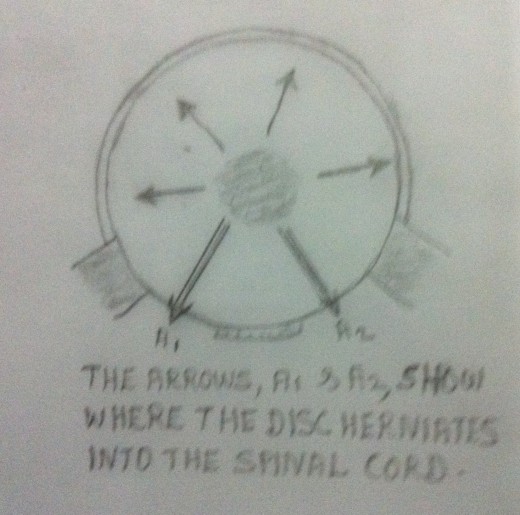
The extrusion of the disc in other directions depends upon it’s attachment to the vertebral ligaments. The disc is loosely attached to the anterior longitudinal ligaments, which in turn is firmly attached to the vertebral bodies. The extrusion of the disc anteriorly or laterally causes anterior or lateral osteophyte formation. Occasionally the osteophyte formation may be so severe that it may unite or fuse two adjacent vertebrae. As a result there may be loss of movement at the apophyseal joints. The disc is more firmly attached to the posterior longitudinal ligaments, which in turn is loosely attached to the posterior aspect of the vertebral bodies. The extrusion of the disc contents posteriorly causes greater problems. In this case the disc extrusion occur postero -laterally. The symptoms may depend on whether the extrusion is acute or whether it occurs slowly or whether it is accompanied by osteophyte formation. In such cases the disc contents and / or the osteophyte growth may press upon the spinal cord and the nerve roots as they travel downwards or through the intervertebral foramina.
Usually a compressive force fractures the vertebral end plate before the force injures the annulus fibrosus. Flexion and extension of the functional unit are well tolerated by the annular fibres.
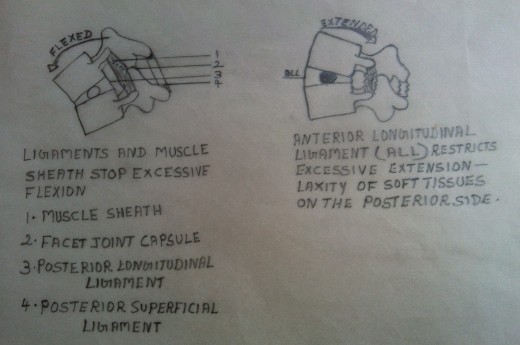
- Excessive flexion is prevented by the Erector Spinae Muscles, posterior longitudinal ligament, posterior superficial ligaments and facet joint capsules.
- The excessive extension is restricted by the mechanical impact of the facet joints and the anterior longitudinal ligaments.
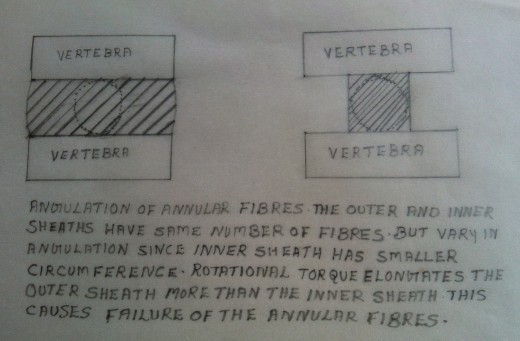
- The excessive rotatory movement is limited by the elongation of the annular collagen fibres of the disc and the mechanical structural limitation posed by the facet joint alignment. Excessive rotational elongation of the annular collagen fibres can disrupt their integrity. There is every chance of annular fibres disruption(or failure) if the rotational movement exceeds 5 degrees. The site of failure varies because of the differences in angulation of the annular fibres. Moreover the length of the annular fibres in the outer sheets of annulus fibrosus is more when compared with the length of the annular fibres in the inner sheets. Since the circumference of the annulus fibrosus is much less in the inner layer than the outer layer, the verticality of the individual fibres differ. The inner fibres are more vertical and hence they do not elongate or stretch as much as the outer fibres on rotation. This accounts for the outer fibres of the annulus fibrosus being torn whenever the rotational forces exceed 5 degrees.
With compression forces, the vertical end plates get closer together with the annular fibres getting further angulated. Fracture of the disc is enhanced by the combination of compression and rotation. With the tearing of the annular fibres of the outer layer, the remaining fibres of the inner layer cannot maintain stiffness. This results in the instability of the functional units of the spine. The contents of the nucleus pulposus get extruded through the weak portions of the annulus fibrosus.
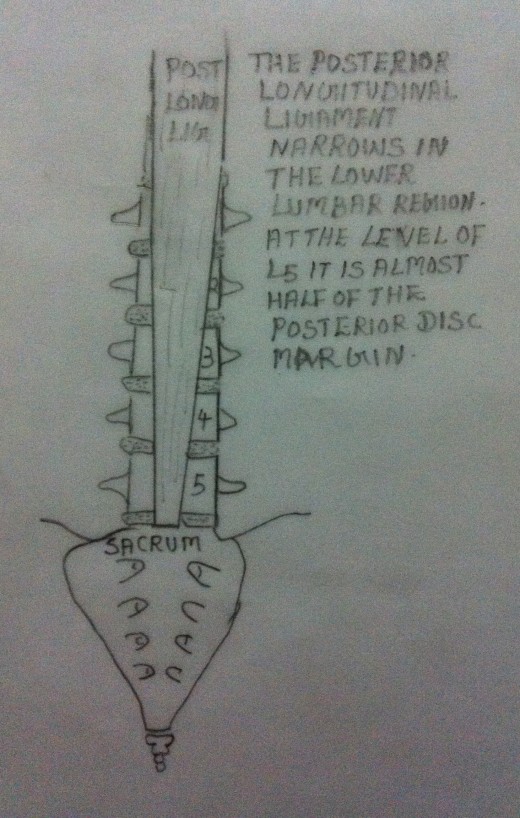
The intervertebral discs are reinforced and protected by the anterior and posterior longitudinal ligaments. These ligaments run the length of the vertebral column anteriorly and posteriorly. They are adherent to the vertebral cortex by the Sharpey Fibres. As they pass by the intervertebral spaces, they are adherent to the outer fibres of the annulus fibrosus. The posterior longitudinal ligament is intact throughout the entire length of the vertebral column until it reaches the lower lumbar region (L3, L4, L5 & S1) where it narrows to half its width. Hence the lower lumbosacral area is always prone to injuries.
The phenomenon of the disc degeneration, with or without osteophyte formation, and extrusion of disc contents is very common. About 60% of the population has significant radiological changes in all the spinal segments, especially in the low back, by the age of 60 years. The incidence of degenerative changes in the spinal segments is higher in men.




